
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Making A Custom Topical Hair Loss Treatment
- Thread starter Swoop
- Start date
- Reaction score
- 950
@Swoop
Check this out: Dynamic Modelling of Pathways to Cellular Senescence Reveals Strategies for Targeted Interventions
Abstract:
They find that inhibition of both ROS with CAT and SOD2, as well as dual mTOR inhibition with Torin1, outperformed either ROS removal or mTOR inhibition alone. They also find that taking down mTOR too far might not be optimal:
The earlier the better:
Unfortunately though, these cells become virtually unrecoverable after a few weeks even with treatment. Do you know how these results might translate to in vivo numbers?
Check this out: Dynamic Modelling of Pathways to Cellular Senescence Reveals Strategies for Targeted Interventions
Abstract:
Cellular senescence, a state of irreversible cell cycle arrest, is thought to help protect an organism from cancer, yet also contributes to ageing. The changes which occur in senescence are controlled by networks of multiple signalling and feedback pathways at the cellular level, and the interplay between these is difficult to predict and understand. To unravel the intrinsic challenges of understanding such a highly networked system, we have taken a systems biology approach to cellular senescence. We report a detailed analysis of senescence signalling via DNA damage, insulin-TOR, FoxO3a transcription factors, oxidative stress response, mitochondrial regulation and mitophagy. We show in silico and in vitro that inhibition of reactive oxygen species can prevent loss of mitochondrial membrane potential, whilst inhibition of mTOR shows a partial rescue of mitochondrial mass changes during establishment of senescence. Dual inhibition of ROS and mTOR in vitro confirmed computational model predictions that it was possible to further reduce senescence-induced mitochondrial dysfunction and DNA double-strand breaks. However, these interventions were unable to abrogate the senescence-induced mitochondrial dysfunction completely, and we identified decreased mitochondrial fission as the potential driving force for increased mitochondrial mass via prevention of mitophagy. Dynamic sensitivity analysis of the model showed the network stabilised at a new late state of cellular senescence. This was characterised by poor network sensitivity, high signalling noise, low cellular energy, high inflammation and permanent cell cycle arrest suggesting an unsatisfactory outcome for treatments aiming to delay or reverse cellular senescence at late time points. Combinatorial targeted interventions are therefore possible for intervening in the cellular pathway to senescence, but in the cases identified here, are only capable of delaying senescence onset.
They find that inhibition of both ROS with CAT and SOD2, as well as dual mTOR inhibition with Torin1, outperformed either ROS removal or mTOR inhibition alone. They also find that taking down mTOR too far might not be optimal:
The model also predicted that an inhibition of mTOR by more than 20% would be sufficient to maintain low mitochondrial mass levels along the time course. Since mitochondrial biogenesis affects the population of new mitochondria, inhibition of mTOR by more than 40% was predicted to be detrimental for this group, compromising healthy cellular function. A safe margin of intervention was predicted to be between 10–20% inhibition, which maintained a moderate and stable population of new mitochondria, and limited the old dysfunctional population.
The earlier the better:
In conclusion, the nature of the biological pathways driving cellular senescence presents a challenge to gaining a sufficient understanding in order to identify novel targeted therapies against the many age-related diseases. A considerable contribution in representing this highly networked biological system and eliciting its properties is offered by mathematical modelling.
Using an integrative systems-biology approach, we determined that multiple interventions for limiting the progression of senescence, and therefore the impact on age-related diseases, are possible: these include down-regulation of ROS and mTOR. Due to the increase in cellular dysfunction over time, these interventions should be applied at early stages and possibly integrated with other interventions aimed at regenerating mitochondria and mitophagy, and reducing inflammation.
Unfortunately though, these cells become virtually unrecoverable after a few weeks even with treatment. Do you know how these results might translate to in vivo numbers?
- Reaction score
- 950
Very good idea, by the way, why not adding grow factors ( you can get minoxidil as powder for cheap, adenosine and KGF as really cheap ( go to skinactives.com for kgf). By the way, a little of tretinoin could be good and a little WNT agonist, like SM. What about the vehicle ?
KGF (FGF7) is already extremely high in Androgenetic Alopecia (6.6 times higher in balding vs. non-balding dermal papilla cells).
Kevand
Established Member
- Reaction score
- 48
we know progesterone is not a 100% hair saver. It might increase T since it blocks 5ar2, but less then finasteride imho.
the study is nice, but 12 patients is not statistically significant...
17-alpha-estradiol is ok until 0,1% by anectdotes and clinical experience. Still, I'm playing it safe an stay on 0,05%.
from my side, no sides. Sometimes I think I have a slightly lower libido some hours after applying it. But, averaging over those many year, it might be libido fluctuations.
2002-2009 I was more or less stable in my mid vertex (front transplanted.. too late to save it in 2002). Then I wanted to improve some thinning areas, and started oral finasteride, until 2015. No dramatic difference, still maintenance. Maybe I wouldn't have maintained with that solution only, and finasteride was key. Or maybe not, who knows.
The compound definetely seems to have the potential to maintain/halt with Ketaconazole and alfatradiol. Although i am sceptical about Progesterone as it also seems anti-estrogenic.
- Reaction score
- 1,332
@WangMQ, yeah that's a problem. Thinking of a way to figure that out. Best would be maybe to do it through someone like Kane or Ziom. They could source each ingredient in bigger quantity. Then we can let them homogenize the ingredients and third party test each ingredient to make sure it's legit. I suppose most of these ingredients are extremely cheap and easy to source aside from DGLA and s-equol which might require custom synthesis, but we'll get there. That way you'll have big quantities of each ingredients that are legit. Now members could buy these ingredients maybe as a "package" for cheap and easily make the solution at home. Every concentration will be open source though so if people want to source it somewhere else or something, they are free to do so obviously.
@Seuxin, yes adenosine and minoxidil would be good.. The thing is you can always add that yourself or use that yourself in combination with this. We can't start with too many ingredients and need to make a choice.We need to start with a basis or it will become too difficult. Like I said all ingredients need to dissolve in a vehicle to make it work. Stability is also an issue if you add much ingredients. I don't even know with certainty if this will fit into one topical. Growth factors are also very high in molecular weight and don't penetrate the skin well and degrade in solution.
@InBeforeTheCure, very interesting. Funny how we unravel more and more and have so much more to learn, I have no clue how this would translate into vivo. However I do seem to think that damage control is very important to shield these cells as much as possible. Reversibility seems to be a hard thing in Androgenetic Alopecia. That's why I aim on damage control with this topical. I have added Tempol as a ROS scavenger into this topical;
Plus check this study http://www.ncbi.nlm.nih.gov/pubmed/22172488. There are many more.
Tempol is rapidly degraded in vivo though. Perhaps application of 2 times per day or more would be better... What do you think of this ingredient? Do you have any idea of other compounds that could combat ROS too efficiently? I was looking at orgotein (SOD) but it's high in MW and poses a problem with delivery. Perhaps we should include a weak mTOR inhibitor too? If so what compound?
Anyway seems to be enough interest. Let's do this then") !
!
@Seuxin, yes adenosine and minoxidil would be good.. The thing is you can always add that yourself or use that yourself in combination with this. We can't start with too many ingredients and need to make a choice.We need to start with a basis or it will become too difficult. Like I said all ingredients need to dissolve in a vehicle to make it work. Stability is also an issue if you add much ingredients. I don't even know with certainty if this will fit into one topical. Growth factors are also very high in molecular weight and don't penetrate the skin well and degrade in solution.
@InBeforeTheCure, very interesting. Funny how we unravel more and more and have so much more to learn, I have no clue how this would translate into vivo. However I do seem to think that damage control is very important to shield these cells as much as possible. Reversibility seems to be a hard thing in Androgenetic Alopecia. That's why I aim on damage control with this topical. I have added Tempol as a ROS scavenger into this topical;
Among several antioxidants currently available, Tempol is a redox-cycling (catalytic), metal-independent, and membrane-permeable antioxidant [57], [58]. It is a particularly attractive molecule because it promotes metabolism of O2− at rates that are similar to SOD and is therefore considered a SOD mimetic; however, Tempol also facilitates metabolism of a wide range of ROS and reactive nitrogen species, including hydroxyl radicals (OH−), and exhibits catalase activity that further prevents generation of OH− and H2O2 by Fenton reactions. Accordingly, Tempol is considered a general-purpose redox-cycling agent rather than a specific SOD mimetic. Tempol improves NO bioavailability and catalytically removes the highly reactive peroxynitrite (ONOO−) species that is produced by the reaction between O2− and NO. Tempol has also been studied in several models of oxidative stress [57], [58]. Of relevance to malaria, Tempol was found to protect many organs—including the brain and the heart—from ischemia/reperfusion injury and improved survival in several models of shock. It also reduces brain or spinal cord damage after ischemia or trauma, among several other effects. In addition, Tempol attenuates the cerebral levels of malondialdehyde and the hippocampal levels of myeloperoxidase caused by cerebral ischemia and reperfusion. Tempol also interferes with metabolism, such as improving insulin response in diabetes, reducing weight gain, lowering blood pressure, and increasing the life span of mice [57], [58]. More recently, Tempol was found to decrease radiation damage and, for this reason, has been used in humans as a topical agent to prevent radiation-induced alopecia[66].
Plus check this study http://www.ncbi.nlm.nih.gov/pubmed/22172488. There are many more.
Tempol is rapidly degraded in vivo though. Perhaps application of 2 times per day or more would be better... What do you think of this ingredient? Do you have any idea of other compounds that could combat ROS too efficiently? I was looking at orgotein (SOD) but it's high in MW and poses a problem with delivery. Perhaps we should include a weak mTOR inhibitor too? If so what compound?
Anyway seems to be enough interest. Let's do this then
!
Last edited:
The compound definetely seems to have the potential to maintain/halt with Ketaconazole and alfatradiol. Although i am sceptical about Progesterone as it also seems anti-estrogenic.
for the little I know, progesterone is the key active ingredient in the compound; 17-alpha-e is the second, then the rest.
ryan82
Established Member
- Reaction score
- 19
Doesnt make S-Eqol makes your scalp "yellow" . I am curious why you use spironolactone? RU is much better ? Respect that you do this!! Goed bezig !
I do not know if you know this forum topic ? But here they also discuss various products / materials to make a topical of .
https://www.baldtruthtaIk.com/threads/22104-Updated-Research-and-Knowledge-Cutting-Edge/
I do not know if you know this forum topic ? But here they also discuss various products / materials to make a topical of .
https://www.baldtruthtaIk.com/threads/22104-Updated-Research-and-Knowledge-Cutting-Edge/
Last edited:
- Reaction score
- 3,660
The compound definetely seems to have the potential to maintain/halt with Ketaconazole and alfatradiol. Although i am sceptical about Progesterone as it also seems anti-estrogenic.
Anti 5-AR and anti-estrogenic.
I still think the ratio of DHT:Estrogen would become more favorable as a result of progesterone, despite it antagonizing estrogen.
In other words the DHT reduction wins out over the reduction in estrogen.
- Reaction score
- 1,332
@ryan82, not that I know of about s-equol making your scalp yellow .
I have roughly calculated. I still need to know the price of DGLA (might require custom synthesis) & Tempol (Tempol is probably extremely cheap). But we are looking at a topical that will be very cheap almost certainly less than $20 a month, that is including every ingredient. Very rough calculation as it depends on concentration of the stuff and frequency of application of the topical and the price of DGLA is still a question mark. spironolactone will be excluded though, that stuff is prescription. Plus it smells like skunk apparently.
You'll still have alfatradiol/s-equol then working on the androgen/ER angle. We'll start with a basis and go from there I guess. Make this a community effort, we can always build from the basis.
.I have roughly calculated. I still need to know the price of DGLA (might require custom synthesis) & Tempol (Tempol is probably extremely cheap). But we are looking at a topical that will be very cheap almost certainly less than $20 a month, that is including every ingredient. Very rough calculation as it depends on concentration of the stuff and frequency of application of the topical and the price of DGLA is still a question mark. spironolactone will be excluded though, that stuff is prescription. Plus it smells like skunk apparently
.You'll still have alfatradiol/s-equol then working on the androgen/ER angle. We'll start with a basis and go from there I guess. Make this a community effort, we can always build from the basis.
Last edited:
ryan82
Established Member
- Reaction score
- 19
Wesley heeft het ooit geprobeerd. Is er mee gekapt omdat het helemaal geel uitslaat... Misschien is er een truucje om dat gele eruit Telogen Effluvium krijgen?@ryan82, not that I know of about s-equol making your scalp yellow
I have roughly calculated. I still need to know the price of DGLA (might require custom synthesis) & Tempol (Tempol is probably extremely cheap). But we are looking at a topical that will be very cheap almost certainly less than $20 a month, that is including every ingredient. Very rough calculation as it depends on concentration of the stuff and frequency of application of the topical and the price of DGLA is still a question mark. spironolactone will be excluded though, that stuff is prescription. Plus it smells like skunk apparently
You'll still have alfatradiol/s-equol then working on the androgen/ER angle. We'll start with a basis and go from there I guess. Make this a community effort, we can always build from the basis.
- Reaction score
- 1,332
Wesley heeft het ooit geprobeerd. Is er mee gekapt omdat het helemaal geel uitslaat... Misschien is er een truucje om dat gele eruit Telogen Effluvium krijgen?
Hmm, ja dat moeten we dan even uitvogelen als dat inderdaad zo is. Hoewel; Appearance: White to Off-White Solid. Btw praat even Engels als je kan, je engels is prima.
They say white to off-white appearance of s-eqoul. Might be a bit beige though. But we'll figure that out.
I.D WALKER
Senior Member
- Reaction score
- 868
I'm seeing a color between off white/ and maybe beige,Hmm, ja dat moeten we dan even uitvogelen als dat inderdaad zo is. Hoewel; Appearance: White to Off-White Solid. Btw praat even Engels als je kan, je engels is prima.
They say white to off-white appearance of s-eqoul. Might be a bit beige though. But we'll figure that out.
concentrating harder on it I'm now thinking it might be buff?
- Reaction score
- 950
@InBeforeTheCure, very interesting. Funny how we unravel more and more and have so much more to learn, I have no clue how this would translate into vivo. However I do seem to think that damage control is very important to shield these cells as much as possible. Reversibility seems to be a hard thing in Androgenetic Alopecia. That's why I aim on damage control with this topical. I have added Tempol as a ROS scavenger into this topical;
Plus check this study http://www.ncbi.nlm.nih.gov/pubmed/22172488. There are many more.
Tempol is rapidly degraded in vivo though. Perhaps application of 2 times per day or more would be better... What do you think of this ingredient? Do you have any idea of other compounds that could combat ROS too efficiently? I was looking at orgotein (SOD) but it's high in MW and poses a problem with delivery
I think you would want to add catalase to take care of the hydrogen peroxide produced by SOD/SOD mimetic. Don't know about the degradation problem. You would probably want round-the-clock inhibition, right?
Perhaps we should include a weak mTOR inhibitor too? If so what compound?
Ideally, you would want a dual mTOR inhibitor. However, these are research chemicals and hard to source, but if you really want it you can get it I suppose. I don't know what kind of concentration you would want to use -- something like AZD8055 has an IC50 of 0.8 nM but a half-life of only 2-3 hours, but I'm not sure how that would translate in practice. It's a double-edged sword with inhibiting mTOR too, since you might end up interfering with stem cell differentiation (rapamycin is known to cause hair loss). Maybe there's some optimal middle ground though, who knows.
KGF (FGF7) is already extremely high in Androgenetic Alopecia (6.6 times higher in balding vs. non-balding dermal papilla cells).
Are you sure ? KGF is in the HSC (Histogen) vial !
- Reaction score
- 4,510
- Reaction score
- 950
Are you sure ? KGF is in the HSC (Histogen) vial !
This is from microarray data (Chew et. al) of dermal papilla cells taken from balding and non-balding scalp. The three on the left (BAB) are balding DPCs, the three on the right (BAN) are non-balding.
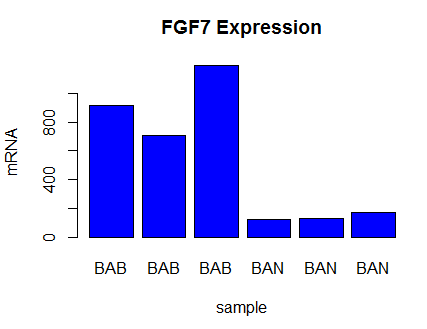
DHT has also been shown to induce FGF7 expression in DPCs. (Kwack et. al, Supplementary Material)
Maybe Histogen could save a few bucks by leaving the FGF7 out lol.