It doesn't matter, if epitestosterone levels are higher when you're preadolescent, then it is in effect a locked door and I guarantee you any research or treatment pathway that focuses on that will be so ungodly expensive that it won't be viable for common consumers.
This is not really an argument, and is akin to saying that because DHT levels decrease as a man gets older, yet his hair loss worsens, that proves that DHT isn't implicated in hair loss. As a research target, control of hormonal synthesis is no less viable than altering prostaglandin pathways or WNT. All of these treatments will be intially expensive, if they even deliver significant results.
What happens with epitestosterone levels in serum as we age is largely irrelevant to what happens in balding hair follicles.
I have quoted you a study where both the
children and their respective
fathers who suffer from androgenic alopecia have a vastly higher ratio of testosterone/epitestosterone in HF compared to controls, showing that the age of the person in question plays very little role and this ratio stays consistent (or gets worse) throughout the lifetime of a patient.
Secondly, here is a study comparing
balding vs
non-balding follicles of the
same person, showing a vast difference in the testosterone/epitestosterone ratio:
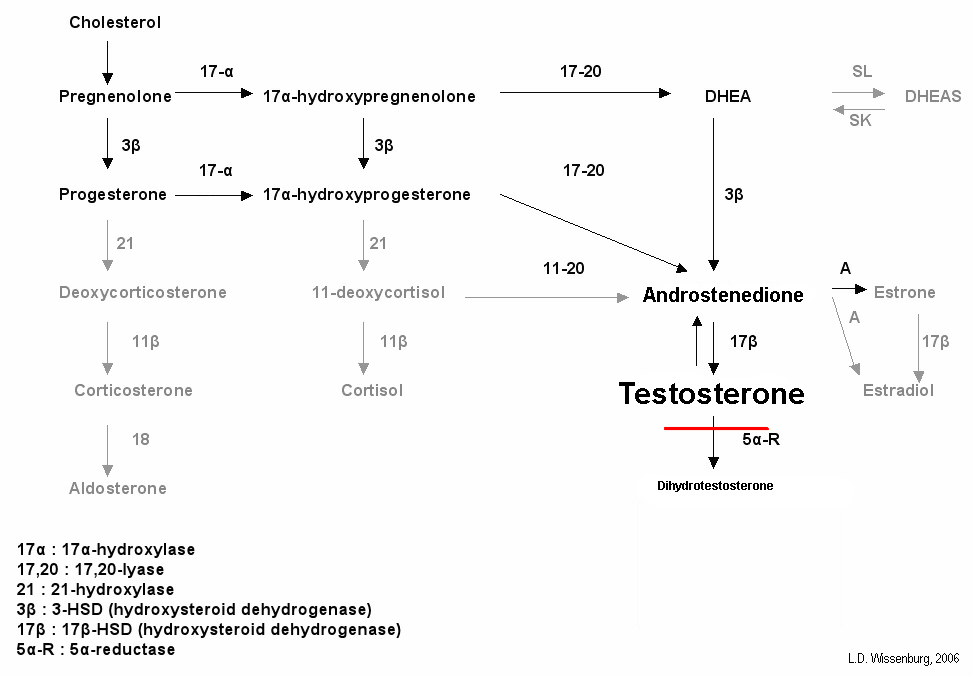
We verified that the distribution of androgenic steroids is unlike in various regions of individual subjects. Moreover, the increased DHT/T ratio in balding plasma indirectly confirms the high activity of 5alpha-reductase type II.

pubmed.ncbi.nlm.nih.gov
The conventional explanation is that occipital (non-balding) follicles simply aren't „sensitive“ to androgens, yet here we see that their hormonal balance is in fact completely different, exhibiting a much lower ratio of androgenic testosterone to its antiandrogenic counterpart epitestosterone, which shows a dramatic difference in local hormone synthesis. This is far more likely to be the explanation for why they aren't 'balding', rather than some mythical lack of androgen sensitivity which has no reasonable means of being quantified.
My hypothesis is that in the case of most men you simply don't need to force your body to emulate the functioning of a prepubescent boy to regrow hair.
Of course not, that is a ridiculous approach, nonetheless employed by some people here. What you need to do is to force your
hair follicles to emulate the functioning of
non-balding hair follicles.
By the time I was 30 I had full regrowth, my hair was about as thick as it was when I was in my teens. There's no way even with my somewhat predisposition for genetic vulnerability to hairloss that somehow magically the testosterone I was exposed to all through my 20s either started or stopped working based on my hair loss or regrowth.
What I can say though is that I believe my estrogen levels were significantly higher, I think that's a far safer assumption than saying a 30 year old man was still retaining high epitestosterone expression in his follicles.
Obviously this is largely anecdotal, but spontaneous regrowth of any kind is rare unless you: had telogen effluvium, some other kind of hormonal imbalance which has resolved (or you have perhaps incurred a 'favorable' one such as increasing your estrogen levels). Without measurements of hormones it is impossible to say anything.
I plan on going the topically applied low dose estrogen route, I will report back my findings, but I have a very strong suspicion that the again relapse hairloss of the last two years I've experienced is due to an imbalance where the ratio of my estrogen to testosterone has faltered and no amount of nuking my DHT levels seems to have helped this.
I have personally used topical estradiolbenzoate for a good while (my results are documented somewhere in the success stories here). Ultimately I had to stop due to side effects, although the results in my case were rather good. As to why nobody else managed to reproduce them, I'm not sure (and a lot of people bought Alpicort F following my experience). Possibly due to the fact that I had gotten off of finasteride a month prior at which point I became hypogonadal or gotten PFS, which would have amplified the results.
My point is that your approach is not exactly ground-breaking, and low dose E2 (esp. In the absence of anti-androgens) will hardly do anything miraculous. Many people have tried that already.