Thanks! I am not a frequent poster, but every now and then I will check this place for video ideas. My video on Cyclosporine for instance was inspired by data I found here.
I am also curious how it could affect retrograde alopecia particularly because retrograde is common even among full density norwood 1-2s and often nonexistent in completely bald norwood 7s, which suggests there are additional factors besides traditional male pattern genetic loss.
The very little that is known about PRLR disruption is that it has been seen to potentially affect hair cycle induction and duration, potentially affect hair texture, and potentially inhibit JAK/STAT signaling, which to my very limited understanding has some effect on follicular cell proliferation and inflammation.
It's possible (likely?) that genetic loss is due to a combination of multiple unrelated attacks on follicular health, and it's possible that the limited success seen by JAK inhibitors in areata could be due to how it alleviates one of those attacks, which could be a vector that some people with genetic loss also suffer from, which explains why regrowth is seen in some people and not others. Also would explain anecdotal evidence from people that say they found some regrowth with anti-inflammatory diets or supplementation, while others did not.
And it's possible that the effects of JAK inhibitors on hair are similar to the effects of the reduction of JAK/STAT signaling from the PRLR clogging of HMI-115 antibodies.
But there's really no way to know how or what the hair-related mechanism behind PRLR blocking is. It could be a glorified JAK inhibitor, but since it is further upstream it could also have some additional beneficial effects. Nobody knows. Nobody will know even if it works, not even the developers of the drug. It's all guesses.
In any case, if it somehow does work, there's a good chance it won't work for most people.
In Alopecia Areata the bulb is destroyed by immune cells. In Androgenetic Alopecia the bulb shrinks over time due to Wnt inhibition caused by AR upregulation. They're not very similar. Actually a lot of signaling in AA and Androgenetic Alopecia is inversely regulated. TGFb1 which is responsible for immune privilege is upregulated in Androgenetic Alopecia while it's downregulated in AA.
Moeman:
“I wouldnt say its 1:1 ratio but definitely as the biomass increases the hormonal levels would be different too.
It could very well be a unique dose to body type style medicine but the trial i was in was purely about safety not dosing regimen. So as such it had to be exactly like the monkey study. I would say 240 will probably yield better results and p3 may even go up again to test for further dosing requirements.
This is all hypothetical and no one knows but the peeps at hope.“
Yes it was 240 over 2 needles of 120, one on each side of the stomach
My apologies it was 6mo ago and im hazy cos i got married at the same time, but again my point was moreso that im much larger than a monkey so efficacy may need bigger doses and that wasnt the prerogative of this trial.
This trial was purely safety. The efficacy regimen is yet to be seen
Moeman:
“I wouldnt say its 1:1 ratio but definitely as the biomass increases the hormonal levels would be different too.
It could very well be a unique dose to body type style medicine but the trial i was in was purely about safety not dosing regimen. So as such it had to be exactly like the monkey study. I would say 240 will probably yield better results and p3 may even go up again to test for further dosing requirements.
This is all hypothetical and no one knows but the peeps at hope.“
Yes it was 240 over 2 needles of 120, one on each side of the stomach
My apologies it was 6mo ago and im hazy cos i got married at the same time, but again my point was moreso that im much larger than a monkey so efficacy may need bigger doses and that wasnt the prerogative of this trial.
This trial was purely safety. The efficacy regimen is yet to be seen
Why this constant cope? Monoclonal antibodies are dosed by lean body mass not how fat you are. Obesity doesn't have a great effect on monoclonal antibody distribution like it does with typical small molecule drugs. Actually, since Moe looks fairly short, his lean body weight is probably on the low end of average, meaning he is actually receiving a high dose for his LBM. Besides, if he was the best responder were they all bigger than him? Rest assured that every patient received a sufficient dose.
For monoclonal antibodies, the distribution volume is limited
to the volume of the blood plasma and extracellular fluids [16,
22]. As a result, body composition is of less importance than
for small molecule drugs, for which volume of distribution is
also determined by adipose, connective, and muscular tissue
[26, 27]. Although blood volume is increased in obese patients
and decreased in underweight patients compared to normal
weight patients, the change in blood volume is less than pro-
portional with the change in body weight [28, 29]. As a result,
total blood volume is better correlated to lean body weight
than to body weight [29].
Based on pharmacokinetic parameters of monoclonal antibodies, there is a rationale for fixed dosing of these drugs in oncology. The currently available knowledge of elimination of monoclonal antibodies combined with the publicly available data from clinical trials and extensive PopPK modeling justifies fixed dosing. Interpatient variation in exposure is comparable after body weight, and fixed dosing and most monoclonal antibodies show relatively flat dose‐response relationships. For monoclonal antibodies, this results in wide therapeutic windows and no reduced clinical efficacy after fixed dosing. Therefore, we believe that fixed dosing at a well‐selected dose can increase medication safety and help in reduction of costs of health care without the loss of efficacy or safety margins.
In Alopecia Areata the bulb is destroyed by immune cells. In Androgenetic Alopecia the bulb shrinks over time due to Wnt inhibition caused by AR upregulation. They're not very similar. Actually a lot of signaling in AA and Androgenetic Alopecia is inversely regulated. TGFb1 which is responsible for immune privilege is upregulated in Androgenetic Alopecia while it's downregulated in AA.
Right, but JAK inhibitors don't work on most areata sufferers, which would suggest any success from JAK inhibition isn't a result of it stopping the immune system from attacking the follicle, and is probably just a result of it reducing the rate at which inflammatory cells created for those attacks reach the follicle.
Though apparently my understanding of the effects PRLR blocking had on JAK inhibition was overstated, because it seems PRLR is only related to JAK2/STAT5 signaling, while the FDA approved JAK inhibitor targets both JAK1 and JAK2.
They don't cure a majority, but they do work to some degree in 80%+ of patients, and give robust growth in over 60%.
One prospective cohort study assessed the efficacyy of tofacitinib at 6 months in 48 patients with AA, and 62.2% patients had achieved at least 50% regrowth of hair after treatment
Several non-randomized clinical trials and retrospective studies have demonstrated encouraging efficacy and well-tolerated safety of tofacitinib in the treatment of alopecia areata. However, there are scarce data on a large cohort of patients with alopecia ...
www.ncbi.nlm.nih.gov
Either way, JAK/STAT signaling is probably not playing a significant causative role in Androgenetic Alopecia, and neither is inflammation which comes only after miniaturization. The dermal papilla is not destroyed in Androgenetic Alopecia, it simply loses its inductive capacity, which in turn makes it shrink, exacerbating the condition.
I think it is a bit presumptuous to claim inflammation has no additive effect on the dermal papilla's ability to induce hair growth. It may not be causative of Androgenetic Alopecia, but it is more than reasonable to believe the resulting introduction of inflammation to that environment assists at least with the vascular dysfunction involved, varying from person to person. Which would explain why not everyone benefits from vasodilators like minoxidil, and again could potentially explain why some people experience anecdotal benefits from anti-inflammatory diets or supplements and others don't.
Clearly HMI-115 isn't a cure and doesn't fix the causative agent behind Androgenetic Alopecia, so if it works in any capacity then it'd only do so by partially relieving the follicular environment from the degenerating factors that are created by whatever is the cause of Androgenetic Alopecia.
The only option is to look for links to the mechanisms behind other known potential hair loss treatments, even non-androgenetic related ones. And it appears there's a link between JAK/STAT and the binding of PRL to PRLR, but obviously we don't know if that link is relevant to its mechanism at all. There's also a link between DHT and increased PRLR mRNA expression, but that might also not be relevant. It could also just be that PRLR disruption reduces the time in telogen, which increases the anagen:telogen ratio of more hairs on the scalp at once, which simply shortens the window in which the inevitable miniaturization occurs.
It's likely none of those things, but they at least appear to have some link. There's no way to know if that link has any impact on the process.
Vasodilation is not how minoxidil promotes hair growth. There are more potent vasoldilators which have no effect on hair growth. Inflammation is generally not helpful but it is moderate in Androgenetic Alopecia, unlike in AA.
I don't put any stock in anecdotal results about diet and supplements. They don't work. Relieving inflammation can help minoxidil work better, but it can't work on its own. Since it is without a doubt not causative in HF miniaturization then relieving it cannot reverse HF miniaturization unless you also counteract the mechanisms which are responsible for inhibiting hair shaft differentiation.
Clearly HMI-115 isn't a cure and doesn't fix the causative agent behind Androgenetic Alopecia, so if it works in any capacity then it'd only do so by partially relieving the follicular environment from the degenerating factors that are created by whatever is the cause of Androgenetic Alopecia.
You could say the same about finasteride, but SRD5A2 is very clearly causative. The fact that it doesn't cure hair loss only means that inhibiting it doesn't reverse all the downstream changes.
There's a link between prolactin and many things involved in hair follicle cycling and Androgenetic Alopecia, but it's too much for me to type right now. There is even an Androgenetic Alopecia risk locus coding for prolactin.
The gene that encodes PRL is located on chr. 6p22.3 and lies within 500 kb of an Androgenetic Alopecia risk locus on the same chromosomal band (lead variant: rs6935891; P = 3.0 × 10−39, β = −0.05, SE = 0.004).
I think you are jumping to conclusions too quickly about the treatment's efficacy and why it does or doesn't work. Let's just wait and see what the trial data shows as it is published. For now we have no trial data and a single anecdote, which is as useless as any finasteride anecdote.
What conclusion was I jumping to? The only possible conclusion one could interpret from what I said is that nobody knows anything. Not me, not you, not the developers of the drug. Even if it works, nobody will know why for many years if ever. It's simply not possible and we can only guess potential links, of which I only listed a few of the countless known and countless more unknown relationships, all of which I said were most likely not related, because nobody actually knows anything.
What is a reasonable conclusion to make is that male pattern baldness often overlaps with other telogen prolonging afflictions, and alleviating those will still increase the anagen to telogen ratio in spite of genetic loss, which will visibly increase the amount of hair on the head despite not stopping the miniaturization of Androgenetic Alopecia, which would explain the many anecdotal stories and pictures of regrowth in male pattern baldness sufferers that aren't on AR inhibitors.
And I think it'd be more precise to say dysregulation of SRD5A2 expression in the follicle is causative, not the gene itself. Though what causes the dysregulation?
But you're right in that there is no point guessing and we should wait for trial data. Though even with positive trial data, we can still only make new guesses as to why it works, since nobody will actually know. So what's the harm in guessing early.
Why this constant cope? Monoclonal antibodies are dosed by lean body mass not how fat you are. Obesity doesn't have a great effect on monoclonal antibody distribution like it does with typical small molecule drugs. Actually, since Moe looks fairly short, his lean body weight is probably on the low end of average, meaning he is actually receiving a high dose for his LBM. Besides, if he was the best responder were they all bigger than him? Rest assured that every patient received a sufficient dose.
What conclusion was I jumping to? The only possible conclusion one could interpret from what I said is that nobody knows anything. Not me, not you, not the developers of the drug. Even if it works, nobody will know why for many years if ever. It's simply not possible and we can only guess potential links, of which I only listed a few of the countless known and countless more unknown relationships, all of which I said were most likely not related, because nobody actually knows anything.
Clearly HMI-115 isn't a cure and doesn't fix the causative agent behind Androgenetic Alopecia, so if it works in any capacity then it'd only do so by partially relieving the follicular environment from the degenerating factors that are created by whatever is the cause of Androgenetic Alopecia.
Like I said, if it worked we would already know. It's really that simple. We would not be relying on a 38 year old disgruntled aussie teasing pics for a revolutionary hair loss treatment.
I'm happy to discuss this with you, but I don't have time for gaslighting. You very clearly have been jumping to conclusions for pages and pages.
You also admitted to being fooled by Brotzu, which throws your judgement into question, and suggests that you are overcompensating now. You formed your judgement on Brotzu based on nothing but emotion because no informed person would have believed in it. Brotzu disappointed you, so now your emotions have swung the other way. 99% of people in this community go through this transition, they go from believing everything will cure them to believing everything is cope. Less than 1% take the time to learn enough to form reasoned judgements on potential treatments.
You're all using the same irrational logic that I even admit to having used during the Brotzu era. It's giving me deja vu.
To drive the point home, you were not using logic then, and you are not now. That was purely an emotional response to your desperation, and this now is purely an emotional response to avoid being fooled again. Maybe HMI turns out to be cope. If it does I will not become emotional over being wrong because there was every reason to believe this treatment had more potential than others. I will continue to approach potential treatments from a logical basis.
What is a reasonable conclusion to make is that male pattern baldness often overlaps with other telogen prolonging afflictions, and alleviating those will still increase the anagen to telogen ratio in spite of genetic loss, which will visibly increase the amount of hair on the head despite not stopping the miniaturization of Androgenetic Alopecia, which would explain the many anecdotal stories and pictures of regrowth in male pattern baldness sufferers that aren't on AR inhibitors.
Telogen prolongation is the least significant effect in male pattern baldness. As you said, telogen duration and A:T ratio has nothing to do with miniaturization, and increasing it only has a minor and temporary cosmetic effect, which isn't even noticeable to the naked eye unless one has telogen effluvium. Telogen effluvium resolves on its own, and is certainly experienced by many people with male pattern baldness. I agree with that part, I just disagree with the conclusion you are drawing that all hair loss has the same overlapping etiology. They factually do not. Scarring alopecias, Androgenetic Alopecia, and AA are all drastically different. Telogen effluvium on its own is of no concern, the hair grows back normally without medication. If you have telogen effluvium and Androgenetic Alopecia, then it will speed up hair loss as hair gets smaller with each hair cycle so anything that promotes catagen earlier will speed it up. In that vein, something like mast cell inhibitors could delay Androgenetic Alopecia progression in part by preventing Telogen Effluvium, but also by preventing release of nasty factors from mast cells like cytokines, substance P and PAI-1. So I mostly agree with you on Telogen Effluvium, but these other conditions are totally unrelated. Retrograde alopecia and DUPA are total unknowns. I don't see any reason to believe they are any different from traditional Androgenetic Alopecia, only the location is different. That could be wrong, but the argument that they are more resistant to treatment doesn't mean much. Some people may just have genetically stronger AR expression in those regions compared to people who typically respond well to finasteride.
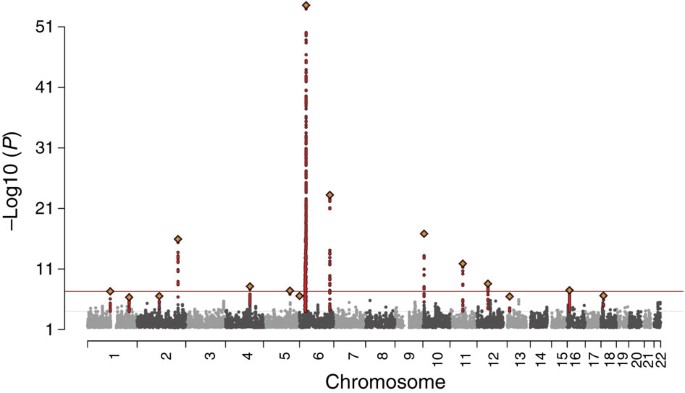
male pattern baldness has virtually no overlap with Alopecia Areata. Just compare the GWAS between the two. Androgenetic Alopecia genes are mostly clustered around AR/EDAR and Wnt, while AA is around immune components.
Alopecia areata (AA) is a common autoimmune disease with a known genetic component. Here, the authors analyse 3,253 AA patients and 7,543 healthy controls, and identify two new risk loci and disrupted immune response pathways associated with the disease.
www.nature.com
In the following image showing differential expression between bald and healthy scalp, the number 1 on the thermometers shows proteins differentially regulated in Androgenetic Alopecia, while number 2 represents those differentially regulated in AA. Every protein here that both diseases have in common is regulated in opposite directions. The biggest problem in Androgenetic Alopecia is that Wnt receptors are downregulated, while in AA they are actually highly upregulated.
These are the top 5 SNPs by P-value found to be causative in AA and then Androgenetic Alopecia. There is no overlap between these SNPs.
This is fine mapping of causal SNPs for various skin traits by cell from a machine learning chromatin analysis. Again, no overlap between AA and Androgenetic Alopecia.
Also there is only one gene, plekhh2, overlapping in that study.
And I think it'd be more precise to say dysregulation of SRD5A2 expression in the follicle is causative, not the gene itself. Though what causes the dysregulation?
Now you're just splitting hairs. There is no requirement for SRD5A2 for hair growth. The gene itself can be CRISPR'd out, and that would completely prevent baldness from ever happening with no obvious side effects. SRD5A2 is higher in bald scalp due to genetics. I take it what you're getting at is how androgen metabolism and the AR becomes upregulated at some point in life. You seem to be implying that only the first domino in the chain can be called causal, but that's not how it works. Every domino in the chain that is required disease initiation has a causal relationship. SRD5A2 has one of the largest, and the fact that knocking it out prevents baldness is proof of that. I'm not aware of any evidence that SRD5A2 expression increases at the time baldness starts. It's upregulated compared to occipital scalp, but is it higher from birth or does it increase with age. I'd say it's probably higher from birth, but it doesn't matter until testosterone production is ramped up during puberty.
So then why do people go bald at different ages? All we can do is speculate about things like cholesterol, CYP17A1/CYP19A1, methylation, Twist 1 or PKC which increase with age, etc. I'd wager it's many things coming together to upregulate the AR locally, and the combination varies from person to person based on their individual genetic background and environment, which also controls when they hit that threshold (different in everyone) where Wnt activation shuts down. Without SRD5A2 to produce DHT it can't happen. Likewise, without the AR it can't happen. Good luck fixing all of the potential mechanisms upstream and downstream of that.
But you're right in that there is no point guessing and we should wait for trial data. Though even with positive trial data, we can still only make new guesses as to why it works, since nobody will actually know. So what's the harm in guessing early.
Now we are in agreement. I have many ideas on how it works, but as you said it's all pure speculation. I will be more interested in speculating on it if it's proven to be as effective as it is in macaques at reversing miniaturization. Those hairs went from full vellus to full terminal. If that happens in humans after a longer time period then it becomes very interesting.
I was referring to the dosing. Clinical trials will not tell because they are not going to trial a higher dose. Phase II participants in China will receive the same 240mg or less. I think they know what dose is required. They have done the pk studies, and they know how monoclonal antibodies work.
I am also curious how it could affect retrograde alopecia particularly because retrograde is common even among full density norwood 1-2s and often nonexistent in completely bald norwood 7s, which suggests there are additional factors besides traditional male pattern genetic loss.
The very little that is known about PRLR disruption is that it has been seen to potentially affect hair cycle induction and duration, potentially affect hair texture, and potentially inhibit JAK/STAT signaling, which to my very limited understanding has some effect on follicular cell proliferation and inflammation.
It's possible (likely?) that genetic loss is due to a combination of multiple unrelated attacks on follicular health, and it's possible that the limited success seen by JAK inhibitors in areata could be due to how it alleviates one of those attacks, which could be a vector that some people with genetic loss also suffer from, which explains why regrowth is seen in some people and not others. Also would explain anecdotal evidence from people that say they found some regrowth with anti-inflammatory diets or supplementation, while others did not.
And it's possible that the effects of JAK inhibitors on hair are similar to the effects of the reduction of JAK/STAT signaling from the PRLR clogging of HMI-115 antibodies.
But there's really no way to know how or what the hair-related mechanism behind PRLR blocking is. It could be a glorified JAK inhibitor, but since it is further upstream it could also have some additional beneficial effects. Nobody knows. Nobody will know even if it works, not even the developers of the drug. It's all guesses.
In any case, if it somehow does work, there's a good chance it won't work for most people.
I understand you need to reconcile the fact that the years and years of time you've spent researching hair loss has amounted to no more utility or understanding than what the average person can surmise from a few hours googling studies.
I'm sure that's a tough pill to swallow and human ego naturally prevents you from accepting it. Trust me I don't envy the position you're in.
But help me understand the point you're trying to make with your quotes of me. Because clearly HMI-115 doesn't cure the cause of Androgenetic Alopecia and no one ever thought it did, right? What's so controversial about that quote? So if it works in any capacity, then it's alleviating any degenerating factors caused by the source of Androgenetic Alopecia. That's a pretty lukewarm take. The earth is also round and the sun is also bright.
And yeah like I said, if HMI-115 caused humans to have the same amount of regrowth as it did in the macaques, we would already know about it. We would not be relying on some 38 year old disgruntled aussie teasing pics. That's pretty much the only conclusion I made that one could even consider being close to a jump.
But how are those two quotes competing thoughts? What qualifies anything I've said as gaslighting? The only gaslighting I'm seeing is from you.
I disagree with the conclusion you are drawing that all hair loss has the same overlapping etiology
When on earth did I say that? I would never imagine claiming that and no reasonable person could possibly interpret what I said was coming even remotely close to that conclusion. Most of the conclusions you think I'm making are being formed in your head. All I said was that male pattern baldness often overlaps with other telogen-prolonging afflictions, which is just a true statement. And any alleviation of those afflictions can give rise to more hair on the head in spite of male pattern baldness, of which we both agree would only be temporary since it does not stop miniaturization. But it could easily explain many anecdotes of regrowth in people with male pattern baldness. If you wanna talk about jumping to conclusions, look in a mirror.
The faulty logic I am more than willing to admit I very temporarily fell for during the Brotzu era were I think pretty basic.
"Why would a world-renowned heart surgeon risk his reputation on a treatment that doesn't work?" etc.
I think in a vacuum that logic is reasonable, but obviously that logic breaks down immediately and becomes irrational as soon as other factors are introduced. And I acknowledge that emotion can give rise to selective attention to create said vacuum. Fortunately for many people, like myself, that is a very temporary state. I have no problems being wrong. I admit when I'm wrong all the time. Most people don't. Especially people who spend years researching a topic that they ultimately will never understand.
Since apparently it's super confusing, let me be incredibly clear:
Neither you or I know anything. Nobody on this forum knows anything. Pictures appeared that suggest regrowth may have occurred, which piqued my interest enough to start trying to form links from available information. Links I constantly made sure to emphasize are complete guesses based solely on available study data and are by all likely accounts entirely unrelated to the actual mechanism at play. As more information appears, I will adjust course accordingly. Pretty standard stuff.
I understand you feel like you're the only one on the forum that's able to make definitive assertions about the mechanisms behind hair loss based on your own conclusions you've drawn from your years of research, and I don't want to take that away from you. Because it would be a complete waste of time for no tangible gain. All those years for nothing. I don't want that. But it seems to be something you hold dear.
Even still, while I'm sure we both agree this back and forth is a waste of time, my primary interest is in speculating whether a new hair loss treatment works or not, which one could easily argue is also a waste of time. But part of me still wants to assuage the vaulted hopes of rubberneckers glancing at this thread. But then I read yet another RolfLeeBuckler comment and I think maybe it's hopeless. Guy is a real life Zoolander.
"Yeah, I wish a black man made a hair loss treatment because there ain't no way a soulful young jazzy jive-cat black man would hustle us, ya dig?" - Acbrantlin 2018
This is what the hair loss industry has been missing. It's the only way they could get our trust back
I'm not reading that whole wall of text, kevin. I can see from the first couple sentences I obviously hurt your feelings. Since you have no argument you resort to ad hominem attacks, a sign of low IQ. That's ok though because your target audience is the low IQ. You have had your hair loss show for a decade now, yet still have not reached a Wikipedia level of understanding, so I guess at this point it's hopeless to discuss anything with you. Good day
I get it. This has been your domain for a very long time and you're free to baselessly call people gaslighters and emotional and it's all kosher, but if anyone returns fire they're breaking the cardinal rule of debate and you automatically win the argument. You can write paragraphs and it's valid, but if anyone else does it it's a flaw. You make up arguments out of thin air to respond to, and if they don't reply to it then you claim they have no argument.
Must be awesome to live above the rules you set for others. It's actually textbook.
But just to really emphasize it, I totally understand that you have to come to terms with the fact that you've spent hundreds and hundreds of hours researching hair loss for no tangible gain and your ego is lashing out trying to rationalize the wasted investment. I don't blame you for that. That's a pretty normal human response. Everyone experiences that at some point. That's why it's important to self-reflect in order to understand others.
"Yeah, I wish a black man made a hair loss treatment because there ain't no way a soulful young jazzy jive-cat black man would hustle us, ya dig?" - Acbrantlin 2018
This is what the hair loss industry has been missing. It's the only way they could get our trust back
I stand by that statement. But this is a hair loss forum so I feel obligated to let everyone know that in that quote I was mocking someone using this thing called sarcasm. The person I was mocking said this: "I just can't see Japanese people as scammers. They're hard working people and more advanced than other countries in a lot of ways. I believe he will do it!" referring to Tsuji.
It shows that I used to be a lot funnier. Unfortunately we all experience change.