
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
New Dermaroller Study; Thoughts, comments?
- Thread starter Jlyncher
- Start date
- Status
- Not open for further replies.
around march i got really lazy and lost a **** load of ground ,end of july i added saBA gel to my regimen,in late august i added dermroller plus growth factors . . anyways here is 2 youtube videos. the first one is multiple snap shot videos throug early sept to sept 21. the next one is from yesterday!!!!
http://www.youtube.com/watch?v=4AfbW0kssIQ&feature=youtu.be
http://www.youtube.com/watch?v=QqVLRC3kMH0
http://www.youtube.com/watch?v=4AfbW0kssIQ&feature=youtu.be
http://www.youtube.com/watch?v=QqVLRC3kMH0
if this smaller hair are all regrowth then GJ on that! NICEaround march i got really lazy and lost a **** load of ground ,end of july i added saBA gel to my regimen,in late august i added dermroller plus growth factors . . anyways here is 2 youtube videos. the first one is multiple snap shot videos throug early sept to sept 21. the next one is from yesterday!!!!
http://www.youtube.com/watch?v=4AfbW0kssIQ&feature=youtu.be
http://www.youtube.com/watch?v=QqVLRC3kMH0
what is saba gel btw?and which growth factors?tell us more about ur regimen,as well as needle frequency and needle lenght
- Reaction score
- 1,063
My theory is that perifollicular fibrosis is really the bad boy of hairloss..
Look at my growing pictures from bald temples, the newborn hairs are coming out of the punctured holes from the derma roller. You see where I am going with this! What his the first step in hair transplantation?
Perifollicular fibrosis: pathogenetic role in androgenetic alopecia.
Yoo HG, Kim JS, Lee SR, Pyo HK, Moon HI, Lee JH, Kwon OS, Chung JH, Kim KH, Eun HC, Cho KH.
Source
Department of Dermatology, Seoul National University College of Medicine, Laboratory of Cutaneous Aging and Hair Research, Clinical Research Institute, Seoul National University Hospital, and Institute of Dermatological Science, Seoul National University, Seoul, Korea.
Abstract
Androgenetic alopecia (Androgenetic Alopecia) is a dihydrotestosterone (DHT)-mediated process, characterized by continuous miniaturization of androgen reactive hair follicles and accompanied by perifollicular fibrosis of follicular units in histological examination. Testosterone (T: 10(-9)-10(-7) M) treatment increased the expression of type I procollagen at mRNA and protein level. Pretreatment of finasteride (10(-8) M) inhibited the T-induced type I procollagen expression at mRNA (40.2%) and protein levels (24.9%). T treatment increased the expression of transforming growth factor-beta 1 (TGF-beta1) at protein levels by 81.9% in the human scalp dermal fibroblasts (DFs). Pretreatment of finasteride decreased the expression of TGF-beta1 protein induced by an average of T (30.4%). The type I procollagen expression after pretreatment of neutralizing TGF-beta1 antibody (10 microg/ml) was inhibited by an average of 54.3%. Our findings suggest that T-induced TGF-beta1 and type I procollagen expression may contribute to the development of perifollicular fibrosis in the Androgenetic Alopecia, and the inhibitory effects on T-induced procollagen and TGF-beta1 expression may explain another possible mechanism how finasteride works in Androgenetic Alopecia.
Article: Perifollicular fibrosis: pathogenetic role in androgenetic alopecia.
Source: Biol Pharm Bull. 2006 Jun;29(6):1246-50.
Author(s): Yoo HG, Kim JS, Lee SR, Pyo HK, Moon HI, Lee JH, Kwon OS, Chung JH, Kim KH, Eun HC, Cho KH
Department of Dermatology, Seoul National University College of Medicine, Laboratory of Cutaneous Aging and Hair Research, Clinical Research Institute, Seoul National University Hospital, and Institute of Dermatological Science, Seoul National University.Summary:
Fibrosis is a scarring process in the skin that can damage the hair follicle (hair loss). This study shows that increased Testosterone speeds up fibrosis while treatment with Finasteride helps slow fibrosis. Stopping or slowing fibrosis may be another method by which Finasteride may help prevent hair loss.
Androgenetic alopecia (Androgenetic Alopecia) is a dihydrotestosterone (DHT)-mediated process, characterized by continuous miniaturization of androgen reactive hair follicles and accompanied by perifollicular fibrosis of follicular units in histological examination. Testosterone (T: 10(-9)-10(-7) M) treatment increased the expression of type I procollagen at mRNA and protein level. Pretreatment of finasteride (10(-8) M) inhibited the T-induced type I procollagen expression at mRNA (40.2%) and protein levels (24.9%). T treatment increased the expression of transforming growth factor-beta 1 (TGF-beta1) at protein levels by 81.9% in the human scalp dermal fibroblasts (DFs). Pretreatment of finasteride decreased the expression of TGF-beta1 protein induced by an average of T (30.4%). The type I procollagen expression after pretreatment of neutralizing TGF-beta1 antibody (10 mug/ml) was inhibited by an average of 54.3%. Our findings suggest that T-induced TGF-beta1 and type I procollagen expression may contribute to the development of perifollicular fibrosis in the Androgenetic Alopecia, and the inhibitory effects on T-induced procollagen and TGF-beta1 expression may explain another possible mechanism how finasteride works in Androgenetic Alopecia.
http://www.derma-haarcenter.ch/files/Directory/News/06_07_2012/EHRS+2012+Barcelona.pdf
Cosmet Dermatol. 2009 Jun;8(2):83-91
Androgenetic alopecia in males: a histopathological and ultrastructural study.
El-Domyati M, Attia S, Saleh F, Abdel-Wahab H.
Department of Dermatology, Faculty of Medicine, Al-Minya University, Al-Minya, Egypt.
Background Androgenetic alopecia is a common cosmetic hair disorder, resulting from interplay of genetic, endocrine, and aging factors leading to a patterned follicular miniaturization. Microinflammation seems to be a potential active player in this process. Aims To study the histopathological and ultrastructural changes occurring in male androgenetic alopecia (Androgenetic Alopecia). Patients/methods Fifty-five subjects were included in this study (40 with Androgenetic Alopecia and 15 as normal age-matched controls). Skin biopsies from frontal bald area and occipital hairy area were subjected to histopathological examination, immunohistochemical staining for collagen I and ultrastructural study. Results The frontal bald area of patients showed highly significant increase in telogen hairs and decrease in anagen/telogen ratio and terminal/vellus hair ratio (P < 0.001). Perifollicular inflammation was almost a constant feature in early cases and showed a significant correlation with perifollicular fibrosis (P = 0.048), which was more marked with thickening of the follicular sheath in advanced cases. Conclusion Follicular microinflammation plays an integral role in the pathogenesis of Androgenetic Alopecia in early cases. Over time, thickening of perifollicular sheath takes place due to increased deposition of collagen, resulting in marked perifollicular fibrosis, and sometimes ends by complete destruction of the affected follicles in advanced cases.
http://www.biomediclaser.com/pdf/Inflammation-in-Androgenetic-Alopecia.pdf
Formation of fibrous tissue or fibroplasia of the dermal sheath, which surrounds the hair follicle, is now suspected to be a common terminal process resulting in the
miniaturization. Involution of the pilosebaceous unit in this form of baldness and sustained microscopic
follicular inflammation with connective tissue remodeling, eventually resulting in permanent hair loss, is
considered a possible cofactor in the complex etiology of androgenetic alopecia. However, till date, the
inflammatory component has not been explored in developing treatment protocols for androgenetic
alopecia.
Fibrosing Alopecia in a Pattern DistributionPatterned Lichen Planopilaris or Androgenetic Alopecia With a Lichenoid Tissue Reaction Pattern?
Patients developed progressive fibrosing alopecia of the central scalp, without the multifocal areas of involvement typical of lichen planopilaris and pseudopelade. Perifollicular erythema, follicular keratosis, and loss of follicular orifices were limited to a patterned area of involvement. Biopsy specimens of early lesions demonstrated hair follicle miniaturization and a lichenoid inflammatory infiltrate targeting the upper follicle region. Advanced lesions showed perifollicular lamellar fibrosis and completely fibrosed follicular tracts indistinguishable from end-stage lichen planopilaris, pseudopelade, or follicular degeneration syndrome.
http://archderm.jamanetwork.com/article.aspx?articleid=189906
INFLAMMATORY PHENOMENA AND FIBROSIS
The implication of microscopic follicular inflammation in the pathogenesis of Androgenetic Alopecia has emerged from several independent studies: An early study referred to an inflammatory infiltrate of activated T cells and macrophages in the upper third of the hair follicles, associated with an enlargement of the follicular dermal sheath composed of collagen bundles (perifollicular fibrosis), in regions of actively progressing alopecia.[25] Horizontal section studies of scalp biopsies indicated that the perifollicular fibrosis is generally mild, consisting of loose, concentric layers of collagen that must be distinguished from cicatricial alopecia.[26] The term 'microinflammation' has been proposed, because the process involves a slow, subtle, and indolent course, in contrast to the inflammatory and destructive process in the classical inflammatory scarring alopecias.[27] The significance of these findings has remained controversial. However, morphometric studies in patients with male pattern Androgenetic Alopecia treated with minoxidil showed that 55% of those with microinflammation had regrowth in response to treatment, in comparison to 77% in those patients without inflammation and fibrosis.[26] Moreover, some forms of primary fibrosing alopecia may represent pathological exaggeration of Androgenetic Alopecia associated with follicular inflammation and fibrosis, specifically postmenopausal frontal fibrosing alopecia,[28] and fibrosing alopecia in a pattern distribution.[29]
An important question is how the inflammatory reaction pattern is generated around the individual hair follicle. Inflammation is regarded as a multistep process which may start from a primary event. Some authors proposed that alopecia may result from cumulative physiological degeneration of selected hair follicles. They described in healthy murine skin clusters of perifollicular macrophages as perhaps indicating the existence of a physiological program of immunologically controlled hair follicle degeneration by which malfunctioning follicles are removed by programmed organ deletion, and suggested that perhaps an exaggerated form of this process might underlie some forms of primary scarring alopecia.[30] The observation of a perifollicular infiltrate in the upper follicle near the infundibulum of human hair follicles in Androgenetic Alopecia suggests that the primary causal event for the triggering of inflammation might occur near the infundibulum.[27] On the basis of this localization and the microbial colonization of the follicular infundibulum with Propionibacterium sp., Staphylococcus sp., Malassezia sp., or other members of the transient flora, one could speculate that microbial toxins or antigens could be involved in the generation of the inflammatory response. Alternatively, keratinocytes themselves may respond to oxidative stress from irritants, pollutants, and UV irradiation, by producing nitric oxide, and by releasing intracellularly stored IL-1α. This pro-inflammatory cytokine by itself has been shown to inhibit the growth of isolated hair follicles in culture. [31] Moreover, adjacent keratinocytes, which express receptors for IL-1, start to engage the transcription of IL-1 responsive genes: mRNA coding for IL-1β, TNFα, and IL-1α, and for specific chemokine genes, such as IL-8, and monocyte chemoattractant protein-1 (MCP-1) and MCP-3, themselves mediators for the recruitment of neutrophils and macrophages, have been shown to be upregulated in the epithelial compartment of the human hair follicle.[27] Besides, adjacent fibroblasts are also fully equipped to respond to such a pro-inflammatory signal. The upregulation of adhesion molecules for blood-borne cells in the capillary endothelia, together with the chemokine gradient, drives the transendothelial migration of inflammatory cells, which include neutrophils through the action of IL-8, T cells, and Langerhans cells at least in part through the action of MCP-1. After processing of localized antigen, Langerhans cells, or alternatively keratinocytes, which may also have antigen presenting capabilities, could then present antigen to newly infiltrating T lymphocytes and induce T-cell proliferation. The antigens are selectively destroyed by infiltrating macrophages, or natural killer cells. On the occasion that the causal agents persist, sustained inflammation is the result, together with connective tissue remodeling, where collagenases, such as matrix metalloproteinase (also transcriptionally driven by pro-inflammatory cytokines) play an active role.[27] Collagenases are suspected to contribute to the tissue changes in perifollicular fibrosis.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2929555/


Thank you Squeegee for enlighting us...
I bold this
"The observation of a perifollicular infiltrate in the upper follicle near the infundibulum of human hair follicles in Androgenetic Alopecia suggests that the primary causal event for the triggering of inflammation might occur near the infundibulum."
Infundibulum is the zone of discharge of sebaceous gland, interesting issue by the way
")
- - - Updated - - -
@squeegee: very informative post, will have to digest all this
Administration of Equol-Producing Bacteria Alters the Equol Production Status in the Simulator of the Gastrointestinal Microbial Ecosystem (SHIME)[SUP]1[/SUP]
http://nutrition.highwire.org/content/136/4/946.full
So basically in the above study they identified the Enterococcus faecium strain as a group of bacterium compable of converting daidzein in the gut into equol. The study below confirms Enterococcus faecium as one of the dominant strains from miso paste.
http://onlinelibrary.wiley.com/doi/10.1046/j.1365-2672.2002.01573.x/full
Thus
1. take soy isoflavones pill containing daidzein,
2. eat miso paste frequently,
3. pray to god it works
On a serious note, there are studies implying that just having a diet rich in isoflavones can turn a non-equol producer into equol producer within months. Some people will scare you that taking high amount of phytoestrogens will give you gyno, or turn you into a woman or some other non-sense like that. Well I have been taking close to 3000mg of phytoestrogens from tea alone (probably contining close to 1000mg of pure EGCG), combining that with close to a 100 mg of phytoestrogens from soy isoflavones, combining with 1280mg of phytoestrogens from curcumin, further I use piperine to increase bioavailability, for almost 8 months now. According to those guys on the internet, I should have a 36 DD by now and breastfeeding my son instead of my wife...
I remember a guy Kofi that talks very well about equol daizein
http://www.disease-treatment.com/showthread.php?t=60621
http://alt.baldspot.narkive.com/52KScBUA/equol-and-fermented-soy-hey-kofi
BTW also allopregnolonone
https://groups.google.com/forum/#!topic/sci.life-extension/n_IKug-rpzU
- - - Updated - - -
Hi guys,
I have been rollering with a 1.5mm 540 needle roller with minoxidil twice a day (except 24 hours post roller) for 5 weeks now and think I can see slight thickening in the places I lost hair the more recently. I am thin at the crown and am hoping in a few months to see my crown looking less thin. I have taken lots of before photos in different light with different lengths of hair so I should have a good baseline. This is my last ditch attempt to recover some hair before I start buzzing it with a 1 guard.
Billy
Good luck
- - - Updated - - -
Congratulations, hair lost recently are more easy to recover.around march i got really lazy and lost a **** load of ground ,end of july i added saBA gel to my regimen,in late august i added dermroller plus growth factors . . anyways here is 2 youtube videos. the first one is multiple snap shot videos throug early sept to sept 21. the next one is from yesterday!!!!
http://www.youtube.com/watch?v=4AfbW0kssIQ&feature=youtu.be
http://www.youtube.com/watch?v=QqVLRC3kMH0
Hopefully a year to see consolidated results.
I think you do not need the dermarroller now
@princessrambo and @squeegee
What do you guys think about Nettle Roots? I have been using it to counter side-effects from finasteride (it blocks aromatase and raises a little bit of T), only for like 15 days now, but it also blocks T conversion to DHT. The thing is, its effect on T to DHT convertion is weak, so i fear that it would actually raise my DHT levels. There is a thread on bodybuilding i guess where some guy said it raised DHT.
I fear i could start loosing hair again if it raises DHT. Most sites and studies i see would point to the opposite, that it lowers, but understanding how it works, and that its DHT conversion blockers are not strong, it could go the other way around.
What do you guys think about Nettle Roots? I have been using it to counter side-effects from finasteride (it blocks aromatase and raises a little bit of T), only for like 15 days now, but it also blocks T conversion to DHT. The thing is, its effect on T to DHT convertion is weak, so i fear that it would actually raise my DHT levels. There is a thread on bodybuilding i guess where some guy said it raised DHT.
I fear i could start loosing hair again if it raises DHT. Most sites and studies i see would point to the opposite, that it lowers, but understanding how it works, and that its DHT conversion blockers are not strong, it could go the other way around.
odalbak
Established Member
- Reaction score
- 11
What do you guys think about Nettle Roots?
Hair roots is what we're talking about here. The mysterious life of follicles.
princessRambo
Established Member
- Reaction score
- 7
LOL, you are a funny guy odaHair roots is what we're talking about here. The mysterious life of follicles.
@super: Where did you see that nettle root inhibits DHT? I can't find a single study stating this, I am just curious, as I haven't come across one yet. From what I know, the mechanism behind its use for BPH is still unclear, but not related to reducing 5AR.
http://www.ncbi.nlm.nih.gov/pubmed/17509841
Only a few components of the active principle have been identified and the mechanism of action is still unclear. It seems likely that sex hormone binding globulin (SHBG), aromatase, epidermal growth factor and prostate steroid membrane receptors are involved in the anti-prostatic effect, but less likely that 5alpha-reductase or androgen receptors are involved.
From what I understand, nettle root competes with DHT to binding to the sex hormone binding globulin. From my understanding, this is NOT a good thing. When free (unbound) SHBG binds to DHT, it effectively makes DHT biologically inactive by preventing it to enter a cell and activate its androgen receptor.
Let's look at this study:
Biological effects of sex hormone-binding globulin on androgen-induced proliferation and androgen metabolism in LNCaP prostate cells.
Addition of purified human SHBG to the medium reduced the effectiveness of DHT on both phases of the proliferative response in a dose-dependent manner. These effects of SHBG appeared to be due primarily to the high affinity binding of DHT by SHBG. Furthermore, analysis of the protein binding of DHT revealed that cell proliferation correlated best with the concentration of DHT not bound to SHBG.
In other words, when they added more SHBG, the free nasty DHT rushed and bounded to it, thus fu*king itself up and preventing it to roam freely and exert its nasty effect on androgen receptors it comes to contact with.
So when the nettle root compounds compete with DHT to bind the SHBG, you can see why that's not a good thing:
The lignan 3,4-divanillyltetrahydrofuran, also present in nettle root was able to completely inhibit DHT from binding to SHBG, yet another indication that it can result in increased free (active) DHT available to tissues such as that in the scalp.
Planta Med. 1997 Dec;63(6):529-32.
Lignans from the roots of Urtica dioica and their metabolites bind to human sex hormone binding globulin (SHBG).
I know there is a lot of people (mostly all Harvard level phd brioscientists) in bodybuilding forums who think they can significantly raise free level of testosterone or dht or what not by using nettle root, but you have to remember that, estrogen, dht, testosterone, etc all compete for SHBG, so you can't pick and choose and say "I just want T to go up". When the amount of free SHBG is low, you likely have high level of unbound estrogen and other hormones as well. This is very speculative and theoretical of course as I am not aware of any study that indicates you can manipulate free (unbound and active) hormone levels in any meaningful way by using nettle root SHBG manipulation.
- - - Updated - - -
I just thought of something, for all the living-on-the-fast-lane guys here, why not try different protocols for different parts of the scalp, like left temple: mild/no blood once a week, right temple: bloody, twice a week, rest of affect area: gory, every 3 weeks or something like that, they you can gauge the most effective way at a personal level
Likely someone else has already posted this info, and I just haven't gotten far enough in the thread to see it....but just in case not....
During pubmed research on a totally different subject last year, I recall seeing, in my search-results, several titles/abstracts talking about cancers from Retin-A. I think the conclusion was that it's a carcinogen.
You might want to do some targeted research on this before deliberately soaking 10-times the normal topical amount into your skin.
Find out what form was least carcinogenic (as I recall, some forms/salts are worse than others), and what dose-level is safe (as I recall, it was a non-linear thing), etc. etc..
I think that one paper mentioned the UK adding a regulation requiring warnings on the bottles...or making certain forms prescription-only....or something along those lines.
I apologize for posting this without links to the papers, but I don't have them...didn't save them back then, because it wasn't germane to me at that time. I just wanted to put this out here before someone soaks their entire scalp with 1000's of mg of a potential carcinogen (assuming that I am recalling correctly).
And perhaps it was a different retinoic-acid derivative that caused the cancers...not "Retin-A".
If so, someone can correct me, and that's fine.
During pubmed research on a totally different subject last year, I recall seeing, in my search-results, several titles/abstracts talking about cancers from Retin-A. I think the conclusion was that it's a carcinogen.
You might want to do some targeted research on this before deliberately soaking 10-times the normal topical amount into your skin.
Find out what form was least carcinogenic (as I recall, some forms/salts are worse than others), and what dose-level is safe (as I recall, it was a non-linear thing), etc. etc..
I think that one paper mentioned the UK adding a regulation requiring warnings on the bottles...or making certain forms prescription-only....or something along those lines.
I apologize for posting this without links to the papers, but I don't have them...didn't save them back then, because it wasn't germane to me at that time. I just wanted to put this out here before someone soaks their entire scalp with 1000's of mg of a potential carcinogen (assuming that I am recalling correctly).
And perhaps it was a different retinoic-acid derivative that caused the cancers...not "Retin-A".
If so, someone can correct me, and that's fine.
As somebody who is still suffering from minoxidil absorption side effects after being off minoxidil for more than two months... Really, do EVERYTHING you can to prevent minoxidil from entering your blood stream. Unless you'd like to speed up your aging.
Guys, all the derma rolling feedback really seems great. And, guess what, there is a way to increase the effectiveness of it drastically: Retin-A. Retin-A is an extremely strong peeling that goes very deep - deep enough to destroy old collagen and induce new collagen formation. In our case, it would destroy the old, hard and fibrotic collagen in the bald areas, and the body will replace it with fresh, soft collagen. Just like derma rolling, except you can reliably cover bigger areas with Retin-A as opposed to only hitting single spots with the rolling.
Combined with the derma rolling, however, the Retin-A would profit from the "tunnels" the way that minoxidil does, and would be delivered directly into our fibrotic collagen.
Retin-A should prove very effective in actually restoring old hair by dissolving fibrotic collagen in bald areas, when combined with derma rolling as it would be able to go deeper instead of just doing its workings at the skin surface.
odalbak
Established Member
- Reaction score
- 11
Retin-A. I think the conclusion was that it's a carcinogen.
Maybe it's not the chemicals involved in the product but the fact that since it's peeling the skin it causes some sort of repeated little inflammation. Adding dermaroller wounding to it would make it worse.
...I may apply an additional strategy: using the roller superficially for like 45-60 min just to break the collagen on every tiny square mm of my scalp.
huh....that one has the ring of 'good idea' to it, odalbak. I'm not qualified to say how much collagen-breaking effect it will have, but I'd expect it to give some of the benefit of 'massage' (as proven beneficial by the Japanese study linked in this thread), and along the lines of the 'Mag-gro' thing. Add in some level of 'collagen disruption', and it seems a good thing.
- - - Updated - - -
.... The study says that after the first wound, there should be another wound done 4mm apart, I think that's good because 4mm is actually kinda of a big gap considering the roller. So in the long run, we should be able to hit adjacent to the first wounds within a few mm....
My take on this is that they may've chosen the 4mm spacing based on the lateral diffusion-distance of minoxidil et al within the epidermis. I'm not saying that I know that distance is 4mm.....I'm suggesting that they may've done tests to determine how far it spreads laterally, and decided that 4mm spacing gives 'full coverage' of the chems...rather than disconnected 'spots' of treatment.
ps; someone posted earlier wondering if follicle grows only where needle enters, or will some follicles also sprout =near= to the treatment 'centers' ? This also ties back to desparatone's (I think it was him) speculation about doing a really serious session less often. I.e., make tens of thousands of wounds all at once....do that once a month. Might save considerable months of time in attaining goal of total head of hair.
- - - Updated - - -
DO, the..ahhh....'thrust'...of that..ahhh...'study'...was to have a cheap source of PGE2. Semen contains PGE2...not FGF9. I don't know the daltons of pge2 offhand, but I think it's considerably smaller than FGF9.
Also, someone else posted that they were mixing it with "lipo-something", presumably a liposome-packaged minoxidil product. I'm not sure how effective that would be. The semen isn't packaged inside the liposomes, so the only amount that would be carried through with them is whatever coated the outside of the 'somes. Likely not much....especially from somewhat dried/gelled semen. That's just my guesstimate.
There might be something to semen after all, but with all things we need to get it absorbed or else it will be useless
http://www.plosone.org/article/info:doi/10.1371/journal.pone.0022564
FGF-9 has a molecular weight of 23,000 dalton. Human skin only allowes about 500 dalton to pass through. Microneedling is supposed to allow up to around 10,000;
http://dermapen.com/micro-needling-drug-delivery/
If you guys really are doing it, then even dermarolling won't help. You'd need to basically strip away skin substantially, a large and wide wound would have to be there in order for FGF-9 to work its magic. Dermabrasion could be it. Another member posted a biopsy punch device on eBay as well, that could work.
Where in the world is rambo anyways, he is the designated translator. He is the one that is suppose to give read all this stuff and summarize it in a neat and ordered fashion
jason5
Member
- Reaction score
- 1
Another Update from me. I feel I'm getting some small regrowth and thickness. Going to do my 9th session today. Here is a comparison pic of week 7 to week 8 (only 1 week difference). Tell me if you see any improvement. I'm going to take a pic every week and post, if you guys are interested in seeing my progress.

squeegee
Banned
- Reaction score
- 131
Androgen Alopecia is a big cluster****.. and yeah the problem seems deeper that what most people think. Biopsies image vertical sectioning.
- - - Updated - - -
Fibroplasia was noted, characterized by an increased number of fibroblasts and increased amounts of collagen around the sebaceous glands and collagenous streamers [ 9 ], in 62% of subjects (Figs. 4 , 5 and 6 ). .
http://www.springerimages.com/Images/MedicineAndPublicHealth/1-10.1007_s00403-003-0447-y-3
- - - Updated - - -
Scalp pathology in androgenetic alopecia: horizontal section. Severe peri-isthmus and peri-sebaceous lymphocytic infiltrates with perifollicular fibrosis (HE ×60)
http://www.springerimages.com/Images/MedicineAndPublicHealth/1-10.1007_s00403-003-0447-y-7
- - - Updated - - -
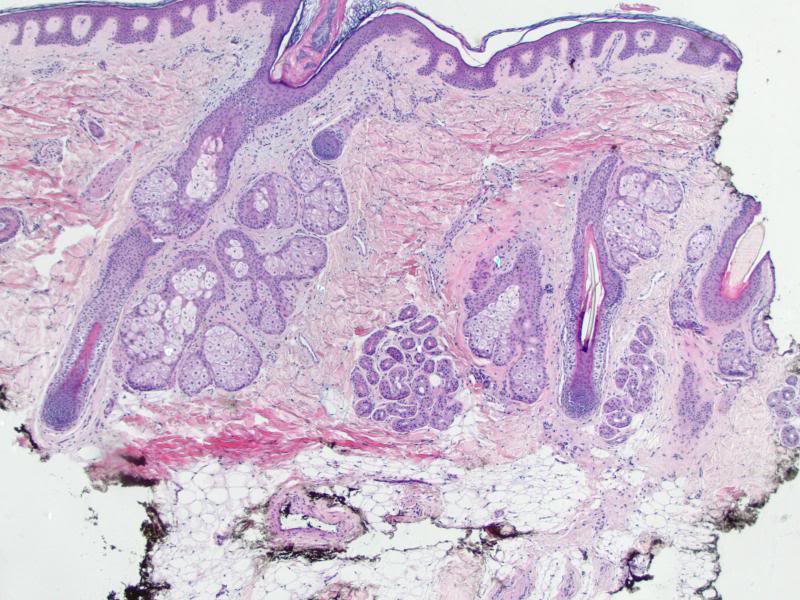
Scalp pathology in androgenetic alopecia: vertical section. Mild perifollicular fibrosis in the dermis (HE ×70)
http://www.springerimages.com/Images/MedicineAndPublicHealth/1-10.1007_s00403-003-0447-y-3
- - - Updated - - -
http://openi.nlm.nih.gov/detailedresult.php?img=2938572_IJT-1-108-g015&req=4
Androgenetic Alopecia is characterized by progressive miniaturization of hair follicles. When the biopsy specimen is sectioned transversely at the level of opening of sebaceous ducts into the hair follicle, the hairs shafts appear vastly different in diameter. The position of the original terminal follicle is indicated by a follicular streamer (stellae or fibrous tract) extending from the subcutaneous tissue up to the course of the follicle to the miniaturized hair. Decreased terminal hairs and increased follicular streamers therefore characterize Androgenetic Alopecia. Sebaceous glands seem enlarged in relation to the miniaturized hair follicles. There is significant reduction in total follicular counts, measured by horizontal sectioning of scalp biopsy. The progressive reduction in the duration of anagen causes a relative increase in telogen hair [Figures 13‐15].
- - - Updated - - -
Some good links for more biopsies pictures..
http://www.dermpedia.org/dermpedia-textbook/androgenic-alopecia
http://www.dermaamin.com/site/histopathology-of-the-skin/53-a/1574-androgenetic-alopecia-.html
- - - Updated - - -
Histological features of peripilar signs associated with androgenetic alopecia.
Deloche C, de Lacharrière O, Misciali C, Piraccini BM, Vincenzi C, Bastien P, Tardy I, Bernard BA, Tosti A.
Source
Centre Charles Zviak, L'Oréal Recherche, 90 rue du Général Roguet, 92583 Clichy Cedex, France. cdeloche@rd.loreal.com
Abstract
BACKGROUND:
A study of the scalp in a large cohort of volunteers with androgenetic alopecia using macrophotographs showed the presence of peripilar signs (PPS) around the hair ostia.
OBJECTIVE:
The aim of the present study was to establish the histopathological features related to PPS.
DESIGN:
Prospective clinicopathological study. SETTING. Department of Dermatology, University Hospital of Bologna.
PATIENTS:
A group of 40 patients (21 males and 19 females) participated in the study. Macrophotographs of the scalp were taken using a Dermaphot camera and PPS were scored using a three-point scale. Hair density and PPS were clinically scored according to reference scales. Two punch biopsies from the photographed area were obtained from each subject and histological analysis was performed on vertical and horizontal sections.
OBSERVATIONS:
Clinical parameters indicated that PPS were already detectable on scalp with high hair density. Moreover, in patients with high hair density (score >4), a significant relationship was found between the PPS score and the global score for perifollicular infiltrates. Thus PPS are linked to superficial perifollicular lymphocytic infiltrates in early androgenetic alopecia.
CONCLUSIONS:
PPS could be the clinical signs reflecting the presence of perifollicular infiltrates.
[h=1]Scalp dermoscopy of androgenetic alopecia in Asian people.[/h]Inui S, Nakajima T, Itami S.
[h=3]Source[/h]Department of Regenerative Dermatology, Graduate School of Medicine, Osaka University, Suita, Osaka, Japan. inui@r-derma.med.osaka-u.ac.jp
[h=3]Abstract[/h]Although dermoscopy is used mainly for diagnosing pigmented skin lesions, this device has been reported to be useful in observing alopecia areata and frontal fibrosing alopecia. Herein, we investigated the dermoscopic features and their incidence of androgenetic alopecia (Androgenetic Alopecia; n = 50 men) and female Androgenetic Alopecia (***A; n = 10 women) in Asian people. More than 20% hair diameter diversity (HDD), which reportedly is an early sign of Androgenetic Alopecia and corresponds to hair follicle miniaturization, was observed in the affected area of all Androgenetic Alopecia and ***A cases, suggesting that HDD is an essential feature to diagnose Androgenetic Alopecia and ***A. Peripilar signs, corresponding to perifollicular pigmentation, were seen in 66% (33/50) of Androgenetic Alopecia and 20% (2/10) of ***A women. This incidence in the present study was lower than previously reported in white subjects possibly because the Asian skin color conceals slight peripilar pigmentation. Yellow dots were observed in 26% (13/50) of Androgenetic Alopecia and 10% (1/10) of ***A cases and the number of yellow dots in Androgenetic Alopecia and ***A was limited to 10 on the overall hair loss area. Yellow dots possibly indicate the coincidence of Androgenetic Alopecia and enlargement of the sebaceous glands caused by common end-organ hypersensitivity to androgen. In conclusion, dermoscopy is useful to diagnose Androgenetic Alopecia and ***A and provides insights into the pathogenesis of Androgenetic Alopecia.

- - - Updated - - -
Fibroplasia was noted, characterized by an increased number of fibroblasts and increased amounts of collagen around the sebaceous glands and collagenous streamers [ 9 ], in 62% of subjects (Figs. 4 , 5 and 6 ). .
http://www.springerimages.com/Images/MedicineAndPublicHealth/1-10.1007_s00403-003-0447-y-3
- - - Updated - - -
Scalp pathology in androgenetic alopecia: horizontal section. Severe peri-isthmus and peri-sebaceous lymphocytic infiltrates with perifollicular fibrosis (HE ×60)
http://www.springerimages.com/Images/MedicineAndPublicHealth/1-10.1007_s00403-003-0447-y-7
- - - Updated - - -
Scalp pathology in androgenetic alopecia: vertical section. Mild perifollicular fibrosis in the dermis (HE ×70)
http://www.springerimages.com/Images/MedicineAndPublicHealth/1-10.1007_s00403-003-0447-y-3
- - - Updated - - -
http://openi.nlm.nih.gov/detailedresult.php?img=2938572_IJT-1-108-g015&req=4
Androgenetic Alopecia is characterized by progressive miniaturization of hair follicles. When the biopsy specimen is sectioned transversely at the level of opening of sebaceous ducts into the hair follicle, the hairs shafts appear vastly different in diameter. The position of the original terminal follicle is indicated by a follicular streamer (stellae or fibrous tract) extending from the subcutaneous tissue up to the course of the follicle to the miniaturized hair. Decreased terminal hairs and increased follicular streamers therefore characterize Androgenetic Alopecia. Sebaceous glands seem enlarged in relation to the miniaturized hair follicles. There is significant reduction in total follicular counts, measured by horizontal sectioning of scalp biopsy. The progressive reduction in the duration of anagen causes a relative increase in telogen hair [Figures 13‐15].
- - - Updated - - -
Some good links for more biopsies pictures..
http://www.dermpedia.org/dermpedia-textbook/androgenic-alopecia
http://www.dermaamin.com/site/histopathology-of-the-skin/53-a/1574-androgenetic-alopecia-.html
- - - Updated - - -
Histological features of peripilar signs associated with androgenetic alopecia.
Deloche C, de Lacharrière O, Misciali C, Piraccini BM, Vincenzi C, Bastien P, Tardy I, Bernard BA, Tosti A.
Source
Centre Charles Zviak, L'Oréal Recherche, 90 rue du Général Roguet, 92583 Clichy Cedex, France. cdeloche@rd.loreal.com
Abstract
BACKGROUND:
A study of the scalp in a large cohort of volunteers with androgenetic alopecia using macrophotographs showed the presence of peripilar signs (PPS) around the hair ostia.
OBJECTIVE:
The aim of the present study was to establish the histopathological features related to PPS.
DESIGN:
Prospective clinicopathological study. SETTING. Department of Dermatology, University Hospital of Bologna.
PATIENTS:
A group of 40 patients (21 males and 19 females) participated in the study. Macrophotographs of the scalp were taken using a Dermaphot camera and PPS were scored using a three-point scale. Hair density and PPS were clinically scored according to reference scales. Two punch biopsies from the photographed area were obtained from each subject and histological analysis was performed on vertical and horizontal sections.
OBSERVATIONS:
Clinical parameters indicated that PPS were already detectable on scalp with high hair density. Moreover, in patients with high hair density (score >4), a significant relationship was found between the PPS score and the global score for perifollicular infiltrates. Thus PPS are linked to superficial perifollicular lymphocytic infiltrates in early androgenetic alopecia.
CONCLUSIONS:
PPS could be the clinical signs reflecting the presence of perifollicular infiltrates.
[h=1]Scalp dermoscopy of androgenetic alopecia in Asian people.[/h]Inui S, Nakajima T, Itami S.
[h=3]Source[/h]Department of Regenerative Dermatology, Graduate School of Medicine, Osaka University, Suita, Osaka, Japan. inui@r-derma.med.osaka-u.ac.jp
[h=3]Abstract[/h]Although dermoscopy is used mainly for diagnosing pigmented skin lesions, this device has been reported to be useful in observing alopecia areata and frontal fibrosing alopecia. Herein, we investigated the dermoscopic features and their incidence of androgenetic alopecia (Androgenetic Alopecia; n = 50 men) and female Androgenetic Alopecia (***A; n = 10 women) in Asian people. More than 20% hair diameter diversity (HDD), which reportedly is an early sign of Androgenetic Alopecia and corresponds to hair follicle miniaturization, was observed in the affected area of all Androgenetic Alopecia and ***A cases, suggesting that HDD is an essential feature to diagnose Androgenetic Alopecia and ***A. Peripilar signs, corresponding to perifollicular pigmentation, were seen in 66% (33/50) of Androgenetic Alopecia and 20% (2/10) of ***A women. This incidence in the present study was lower than previously reported in white subjects possibly because the Asian skin color conceals slight peripilar pigmentation. Yellow dots were observed in 26% (13/50) of Androgenetic Alopecia and 10% (1/10) of ***A cases and the number of yellow dots in Androgenetic Alopecia and ***A was limited to 10 on the overall hair loss area. Yellow dots possibly indicate the coincidence of Androgenetic Alopecia and enlargement of the sebaceous glands caused by common end-organ hypersensitivity to androgen. In conclusion, dermoscopy is useful to diagnose Androgenetic Alopecia and ***A and provides insights into the pathogenesis of Androgenetic Alopecia.
odalbak
Established Member
- Reaction score
- 11
Horizontal sections remind me of andouillette slices.
I'd like to see biopsies of healthy scalp and compare. But it looks like fibrosis is investing the whole scalp. That makes the hypothesis of scalp massage therapy more credible. One needs to break that hardened matter everywhere.
I'd like to see biopsies of healthy scalp and compare. But it looks like fibrosis is investing the whole scalp. That makes the hypothesis of scalp massage therapy more credible. One needs to break that hardened matter everywhere.
princessRambo
Established Member
- Reaction score
- 7
From what I see the scalp seems a little less palish (which can be a sign of good things happening down under, or a nice tanAnother Update from me. I feel I'm getting some small regrowth and thickness. Going to do my 9th session today. Here is a comparison pic of week 7 to week 8 (only 1 week difference). Tell me if you see any improvement. I'm going to take a pic every week and post, if you guys are interested in seeing my progress.
), a week isn't enough to see if thicker growth is occurring from this distance unless you use microscopic photographic technology like they did in the dermaroller study. Keep'em coming, do you have week 1 pics?Manoko For some reason, I can't access the last page of this thread (Page 145).
Weird.
Edit: problem solved, apparently this page didn't exist yet. Now it does thanks to you. Lol. Funniest thing ever. Anyway I have been rolling for 6weeks and doing minoxidil. IF I get results I will post pics.
Weird.
Edit: problem solved, apparently this page didn't exist yet. Now it does thanks to you. Lol. Funniest thing ever. Anyway I have been rolling for 6weeks and doing minoxidil. IF I get results I will post pics.
odalbak
Established Member
- Reaction score
- 11
What i'd like to see is a progressing hairline (as opposed to receding). This is the ultimate challenge. When that happens the last skeptics will blush like dermarolled scalps. Stopping deforestation is great but we need all our sacred trees back. Let's dig holes in this devastated soil.
isishearmyplea
Experienced Member
- Reaction score
- 42
What i'd like to see is a progressing hairline (as opposed to receding). This is the ultimate challenge. When that happens the last skeptics will blush like dermarolled scalps. Stopping deforestation is great but we need all our sacred trees back. Let's dig holes in this devastated soil.
do you have any idea if the new follicles will be susceptible to DHT?? I want get on this rolling thing but i am NW1.5-2.5 and i dont know whether rolling will **** my existing follicles. or am i supposed to roll in the area where i have lost hair, and using it at the thinning area also seems scary.
zombiehair
Member
- Reaction score
- 3
Hey jason5
I wonder If the contrasting redder blotchy areas of your scalp are the pebbled appearance mentioned in the four stages of healing squeegee had posted earlier in the thread.
I have noticed this pebbling appearance on the photos squeegee posted as well as my own head.
Thoughts anyone ?
I'm about to put myself through roll 6 .That's about 8 days since my last session.
I wonder If the contrasting redder blotchy areas of your scalp are the pebbled appearance mentioned in the four stages of healing squeegee had posted earlier in the thread.
I have noticed this pebbling appearance on the photos squeegee posted as well as my own head.
Thoughts anyone ?
I'm about to put myself through roll 6 .That's about 8 days since my last session.
- Status
- Not open for further replies.