
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Gene Therapy - Fixing Single Nucleotide Polymorphisms to cure PGD2 sensitivity
- Thread starter macaroni
- Start date
- Reaction score
- 950
This poster perfectly describes three SNPs in the CRTH2/DP2 gene that are found in individuals that have PGD2 sensitivity. Those who suffer from hairloss, have PGD2 sensitivity, so since these SNPs have been identified, and the method for gene therapy has been determined, i don't see a reason why gene therapy can't be used to fix the three SNPs (rs545659, rs634681, and rs7167) responsible for PGD2 sensitivity.
That's not what the poster says. All the tissue samples are from people with hair loss, but some of them weren't affected by PGD2, at least in terms of hair length.
The obvious gene therapy target for us would be AR, at least to start with.
- Reaction score
- 1,332
That's not what the poster says. All the tissue samples are from people with hair loss, but some of them weren't affected by PGD2, at least in terms of hair length.
The obvious gene therapy target for us would be AR, at least to start with.
Indeed. To hell with PGD2. It's highly likely that it doesn't even play a big role in Androgenetic Alopecia imo.
The AR is the major player in Androgenetic Alopecia and needs to be eliminated. Eliminate the AR and Androgenetic Alopecia is gone, simple as that. Locally only obviously
") .
.- - - Updated - - -
Can you guys point me to the AR studies that confirm what you are claiming? I want to study up on that so i can better understand it
Thanks
What specifically? The importance of the AR in relation to Androgenetic Alopecia?
"Setipiprant previously been studied as a potential allergic inflammation treatment and had undergone eight clinical trials, resulting in a safety database of more than 1,000 patients".
If they have not seen any regrowth back then that could mean that seti is useless for hairloss or as swoop says PGD2 has nothing to do with hairloss.
If they have not seen any regrowth back then that could mean that seti is useless for hairloss or as swoop says PGD2 has nothing to do with hairloss.
- Reaction score
- 950
Indeed. To hell with PGD2. It's highly likely that it doesn't even play a big role in Androgenetic Alopecia imo.
The AR is the major player in Androgenetic Alopecia and needs to be eliminated. Eliminate the AR and Androgenetic Alopecia is gone, simple as that.
Well, significant Ptgds upregulation is damaging to hair follicles. It's a "secondary" effect of AR activity in DP cells though, and there are many of these bad secondary effects, so yeah, I think eliminating PGD2 alone is very unlikely to stop Androgenetic Alopecia. If it's true that some people with hair loss aren't even affected by PGD2, as that poster Hellouser posted says, that would confirm this. But there are many of these secondary effects that can hurt you, and lopping off the tentacles of the male pattern baldness hydra is a frustrating endeavor. Anyone who doubts this should go read an Eldarlmario thread.
Unfortunately, it seems like most hair loss researchers are focused exclusively on these secondary effects, and very little research has been done into AR dynamics in Androgenetic Alopecia and why these effects arise.
Swoop said:Locally only obviously
Choose your gene therapy doctor carefully!

- Reaction score
- 1,332
Well, significant Ptgds upregulation is damaging to hair follicles. It's a "secondary" effect of AR activity in DP cells though, and there are many of these bad secondary effects, so yeah, I think eliminating PGD2 alone is very unlikely to stop Androgenetic Alopecia. If it's true that some people with hair loss aren't even affected by PGD2, as that poster Hellouser posted says, that would confirm this. But there are many of these secondary effects that can hurt you, and lopping off the tentacles of the male pattern baldness hydra is a frustrating endeavor. Anyone who doubts this should go read an Eldarlmario thread.
Unfortunately, it seems like most hair loss researchers are focused exclusively on these secondary effects, and very little research has been done into AR dynamics in Androgenetic Alopecia and why these effects arise.
In what way is it damaging though? What did Cotsarelis really show? He did show that PGD2 is upregulated in the balding scalp right. But is that really a big thing? Not at all, as there are a plethora of other factors that are upregulated in the balding scalp (P53, DKK-1, MMP's, Caspase's, ETC....)
Furthermore he has shown that PGD2 stops or slows hair growth in a hair follicle vitro model. The thing here is that extremely many compounds can perform exactly the same action if not better on a hair follicle in vitro model. Is a hair follicle in vitro model also a good model? No, obviously not.
So like you mention we can call PGD2 a secondary event that happens somewhere downstream. But first of all is this particular event unique to Androgenetic Alopecia? Do only people with Androgenetic Alopecia suffer from enhanced PGD2 levels in their scalp?
We have known that prostaglandines are involved in (healthy) hair follicle cycling since the 90's. But many factors are involved in normal hair follicle cycling. Some will be expressed with the telogen or catagen phase, and others will be expressed with the anagen phase. After all the healthy hair follicle is a little dynamic organ that cooperates with the environment.
Prostaglandines also work primarily in a autocrine/paracrine fashion I think? Anyway, mast cells are the main thing that synthesize PGD2 in the human body. In fact, not a long while ago it was also thought that mast cells were prtty much exclusively the only cells that produced PGD2, however this has recently been challenged.
Mast cells itself have their function in hair follicle cycling too. They are enhanced in the telogen phase and decline in the anagen phase.
Now in relation to mast cells and Androgenetic Alopecia, we also see that mast cells increase significantly. The funny thing is.. This isn't unique to Androgenetic Alopecia it seems;
There are also clinical indications that MC may be involved in the pathogenesis of several human hair growth disorders. In some forms of scarring alopecias (32-34) and in androgenetic alopecia (35), the number of skin MC is reportedly increased. Degranulation of perifollicular MC and activation of fibroblasts in the direct vicinity of these MC may be seen around hair follicles that are in the earliest stages of undergoing the androgen-dependent transformation front terminal to
vellus hair follicles in male pattern baldness (36). In addition, early lesions of alopecia areata may show a numeric MC increase (37, 38),
So why didn't we for instance see research on PGD2 levels on people with other hair growth disorders? That would be interesting.
But let's hypothetically assume that the increase of PGD2 levels is unique to Androgenetic Alopecia.
Now let's assume we take a group of people who have Androgenetic Alopecia and we castrate them. So their balding stops right as Androgenetic Alopecia is androgen dependent. Now we are going to blast them with PGD2. In this case would PGD2 still cause the same actions that primarily were induced by the androgens? Would it cause miniaturization and lead to eventual arrest? In my opinion most probably not. "Androgenetic Alopecia" wouldn't be Androgenetic Alopecia anymore in this case and PGD2 might still be harming but in a different way if that makes sense.
After all people who don't suffer from Androgenetic Alopecia can still lose their hair by compounds too. Look at SHH antagonists for example. They induce in almost every case severe alopecia, which may even be permanent or very long lasting. Still that isn't due to Androgenetic Alopecia but simply because of using a SHH antagonist. And who says that their PGD2 levels won't increase because of the SHH antagonist?
Back to mast cells again, there is also high evidence that they are implicated in tissue remodeling in the body. Well guess what whether one loses hair due to a pathology or whether a healthy hair follicle goes into telogen, the tissue will need to remodel.
This goes back obviously if PGD2 levels are indeed unique to Androgenetic Alopecia but even if it was the other question stands.
However ultimately we can clearly see that even the strongest DP2 antagonists don't seem to provide significant cosmetic changes. I mean take 100 people who all suffer from some sort of degree of Androgenetic Alopecia and place them on dutasteride. A percentage of them will have surely significant cosmetic changes.
This point alone tells me immediately that PGD2 is simply not a major player in the pathology of Androgenetic Alopecia.
The AR however is obviously a major player. And that's what we need to focus on. Speaking in terms of gene therapy we might be lucky as the AR seems to function as a central role in prostate cancer too
. Hopefully we can benefit from these advancements;- AZD5312, a generation 2.5 antisense oligonucletotide targeting the androgen receptor
https://clinicaltrials.gov/ct2/show/NCT02144051
These antiandrogen antisense oligonucleotides can downregulate the AR expression. Designed antisense oligonucleotides inhibit AR protein levels targeting new disclosed antisense sensitive regions on the AR transcript. Androgenetic alopecia, acne and other androgen-related dermatological disorders are still waiting for treatments which should be more effective, specific, and safe. Antisense oligonucleotide biotechnology should provide more specific and less toxic therapy.
unk:- Reaction score
- 6,429
The AR however is obviously a major player. And that's what we need to focus on. Speaking in terms of gene therapy we might be lucky as the AR seems to function as a central role in prostate cancer too
- AZD5312, a generation 2.5 antisense oligonucletotide targeting the androgen receptor
Do you think a drug like this, which focuses on downregulation of AR, would be more beneficial for our purposes than traditional AAs like RU? And how do you think they would compare in terms of safety? AR half-life is around 6-15 hours right so I guess this would need to be twice daily topical at least.
- Reaction score
- 11,943
Swoop,
You're the most informed among the active posters on this forum.
You make a compelling case that it's all about androgens.
But the fact is a huge number of men have really high testosterone/DHT levels and never get Androgenetic Alopecia. It's not just androgens. There's an extra hidden variable, that may be more beneficial than castration.
You're the most informed among the active posters on this forum.
You make a compelling case that it's all about androgens.
But the fact is a huge number of men have really high testosterone/DHT levels and never get Androgenetic Alopecia. It's not just androgens. There's an extra hidden variable, that may be more beneficial than castration.
- Reaction score
- 1,332
Do you think a drug like this, which focuses on downregulation of AR, would be more beneficial for our purposes than traditional AAs like RU? And how do you think they would compare in terms of safety? AR half-life is around 6-15 hours right so I guess this would need to be twice daily topical at least.
I can't seem to find anything about that specific drug. Anyway from what I know, antisense gene therapy "silences" the gene. In this case it would destroy the AR mRNA. Because of this the AR protein can't be formed as it depends on AR mRNA to build itself.
The benefit of this is that when done properly that it should only act on the cells/tissue that you want to target. So if we could target the scalp only that would make that place just pretty much completely devoid of AR. Our scalp would live the eunuch lifestyle while the rest of our body has normal AR function. It would fix the sensitivity issue, our cells would be fully or nearly non responsive to androgens.
As far as I know you wouldn't be needing to apply this daily but only deliver it to the target cells and then maintain the cells with the stuff once in a while. I have read that this stuff can stay active for longer than a half year, especially with the new recently generation therapies.
Here is some good quick general information actually about antisense therapy; http://www.medibiztv.com/articles/the-antisense-gene-therapy
Vitravene for instance that is already on the market requires a initial dosage and then a maintenance dosage every 4 weeks.
Like I quoted a while ago difference vertex balding and occipital healthy dermal papilla cells
To identify differences in the transcription of AR in defined two sites, their mRNA levels were examined. In all samples, mean mRNAs of AR were 3.4- fold higher in vertex dermal papilla cells than those from occipital scalp
I hope we can benefit man from this in the future.
- - - Updated - - -
You make a compelling case that it's all about androgens.
But the fact is a huge number of men have really high testosterone/DHT levels and never get Androgenetic Alopecia. It's not just androgens. There's an extra hidden variable, that may be more beneficial than castration.
Well what about genes? How many studies have outlined the importance of the androgen receptor gene in relation to androgenetic alopecia? Countless! We are unlucky with the inheritance of our genes, some are more lucky. Go read the Hamilton studies.
I don't get what you mean by "it's not just androgens". If everyone would be castrated at a young age on this forum everyone would retain his hair pre-balding and not suffer from Androgenetic Alopecia. Androgenetic Alopecia is dependent on androgens, no wonder as androgens need to exert their biological function through the androgen receptor. Androgens > AR.
I don't see how anything can be more beneficial against Androgenetic Alopecia than total androgen ablation or removal of the AR. Castration stops the progression of Androgenetic Alopecia, so it eliminates the chain of Androgenetic Alopecia.
If we can get gene therapy on our scalp that destroys the AR then that would be the best therapy ever man. Nobody would ever have to suffer from Androgenetic Alopecia again, it's that simple.
Indeed it won't yield reversal of Androgenetic Alopecia, but reversal of Androgenetic Alopecia is something else. Instead of stopping the chain (prevention) you are trying to reverse the action or damage that has been done already. Now that is on a whole different level right..
If you were to be castrated at a young age you wouldn't be here man. You would retain your hair pre-balding.. We all would.
farkhairloss
Established Member
- Reaction score
- 37
Swoop, I have read many of your posts, you have a medical background I remember reading. I have also read about DIY gene therapy. Im not blowing wind up your *** but you and a few of the other intellects on this forum should be looking into this. SERIOUSLY!
TheNothing85
New Member
- Reaction score
- 1
I need 4 posts to start a new thread
Swoop!
Swoop!
- Reaction score
- 6,429
I can't seem to find anything about that specific drug. Anyway from what I know, antisense gene therapy "silences" the gene. In this case it would destroy the AR mRNA. Because of this the AR protein can't be formed as it depends on AR mRNA to build itself.
The benefit of this is that when done properly that it should only act on the cells/tissue that you want to target. So if we could target the scalp only that would make that place just pretty much completely devoid of AR. Our scalp would live the eunuch lifestyle while the rest of our body has normal AR function. It would fix the sensitivity issue, our cells would be fully or nearly non responsive to androgens.
As far as I know you wouldn't be needing to apply this daily but only deliver it to the target cells and then maintain the cells with the stuff once in a while. I have read that this stuff can stay active for longer than a half year, especially with the new recently generation therapies.
Here is some good quick general information actually about antisense therapy; http://www.medibiztv.com/articles/the-antisense-gene-therapy
Vitravene for instance that is already on the market requires a initial dosage and then a maintenance dosage every 4 weeks.
Like I quoted a while ago difference vertex balding and occipital healthy dermal papilla cells
I hope we can benefit man from this in the future.
Interesting stuff brah, thanks.
I'm wondering why hairloss researchers haven't pursued the angle further, but I see that AZD drug is "first-in-class" so I assume drugs with this mechanism are still cutting edge. Silencing or at least significantly impairing AR expression in the scalp would completely kill the progression of Androgenetic Alopecia. Lets hope we see more trials being conducted on this class of drugs, because obviously the safety profile would be the biggest concern. Hopefully in the near future we could use this ourselves, much like when RU58841 came on the scene all those years ago.
- Reaction score
- 1,332
Interesting stuff brah, thanks.
I'm wondering why hairloss researchers haven't pursued the angle further, but I see that AZD drug is "first-in-class" so I assume drugs with this mechanism are still cutting edge. Silencing or at least significantly impairing AR expression in the scalp would completely kill the progression of Androgenetic Alopecia. Lets hope we see more trials being conducted on this class of drugs, because obviously the safety profile would be the biggest concern. Hopefully in the near future we could use this ourselves, much like when RU58841 came on the scene all those years ago.
Exactly my thoughts brah, let's hope for the best
.- Reaction score
- 950
In what way is it damaging though? What did Cotsarelis really show? He did show that PGD2 is upregulated in the balding scalp right. But is that really a big thing? Not at all, as there are a plethora of other factors that are upregulated in the balding scalp (P53, DKK-1, MMP's, Caspase's, ETC....)
Furthermore he has shown that PGD2 stops or slows hair growth in a hair follicle vitro model. The thing here is that extremely many compounds can perform exactly the same action if not better on a hair follicle in vitro model. Is a hair follicle in vitro model also a good model? No, obviously not.
So like you mention we can call PGD2 a secondary event that happens somewhere downstream. But first of all is this particular event unique to Androgenetic Alopecia? Do only people with Androgenetic Alopecia suffer from enhanced PGD2 levels in their scalp?
We have known that prostaglandines are involved in (healthy) hair follicle cycling since the 90's. But many factors are involved in normal hair follicle cycling. Some will be expressed with the telogen or catagen phase, and others will be expressed with the anagen phase. After all the healthy hair follicle is a little dynamic organ that cooperates with the environment.
Prostaglandines also work primarily in a autocrine/paracrine fashion I think? Anyway, mast cells are the main thing that synthesize PGD2 in the human body. In fact, not a long while ago it was also thought that mast cells were prtty much exclusively the only cells that produced PGD2, however this has recently been challenged.
Right. In Androgenetic Alopecia, AR causes a shift in gene expression and number of DP cells that alters communication between DP and the epithelial HF, and there are many damaging changes.
Swoop said:Mast cells itself have their function in hair follicle cycling too. They are enhanced in the telogen phase and decline in the anagen phase.
If that's the case, they actually have the opposite pattern to Ptgds expression in HFs. Based on the data I have*, Ptgds rises during anagen, peaks in mid-to-late anagen, and is actually lowest in late catagen and telogen (following catagenic apoptosis of the epithelial HF cells expressing Ptgds, I suppose).
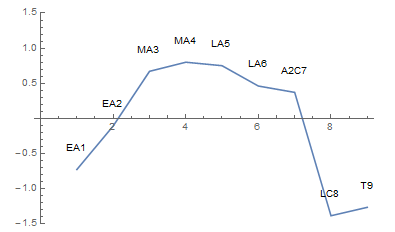
EA = early anagen, MA = mid anagen, LA = late anagen, A2C = anagen to catagen transition, LC = late catagen, T = telogen
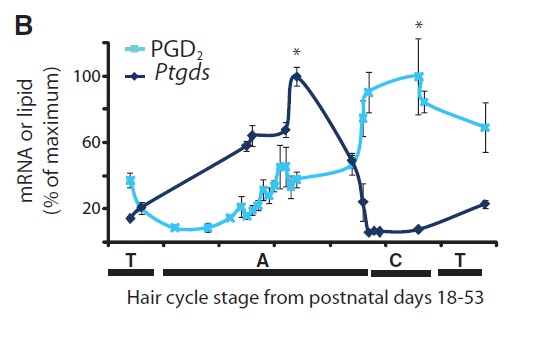
Cotsarelis found something similar:
* Gene expression data for several thousand genes through the hair cycle in mice is available here.
Swoop said:Now in relation to mast cells and Androgenetic Alopecia, we also see that mast cells increase significantly. The funny thing is.. This isn't unique to Androgenetic Alopecia it seems;
So why didn't we for instance see research on PGD2 levels on people with other hair growth disorders? That would be interesting.
I don't know of any research on that. There's this paper on alopecia areata. There are some similarities in gene expression to Androgenetic Alopecia -- decreased expression of HF structural proteins (trivial), increased cytokine production, DNA repair markers, cell cycle genes, downregulation of anti-apoptotic genes, but differences also (immunity markers in particular). It looks like they didn't test Ptgds expression, unfortunately.
EDIT: I was looking at Supplemental Table 1, which is a list only of statistically significant differentially expressed genes, so if they tested it, Ptgds isn't on it. Sadly they didn't provide the raw data...
Swoop said:But let's hypothetically assume that the increase of PGD2 levels is unique to Androgenetic Alopecia.
Now let's assume we take a group of people who have Androgenetic Alopecia and we castrate them. So their balding stops right as Androgenetic Alopecia is androgen dependent. Now we are going to blast them with PGD2. In this case would PGD2 still cause the same actions that primarily were induced by the androgens? Would it cause miniaturization and lead to eventual arrest? In my opinion most probably not. "Androgenetic Alopecia" wouldn't be Androgenetic Alopecia anymore in this case and PGD2 might still be harming but in a different way if that makes sense.
I think it would, actually, at least in the "PGD2-sensitive" people. As I posted here, PGD2/CRTH2 can promote the nuclear translocation of NFATc1, which binds to the CDK4 promoter in bulge stem cells and represses its transcription. This stops G1/S cell cycle progression. NFATc1 can also bind to Dvl in the nucleus, which represses beta-catenin transcriptional activity.
Also, those transgenic mice overexpressing Cox2 quoted in the Cotsarelis paper had HF miniaturization and sebaceous gland hyperplasia (beta-catenin controls keratinocyte cell fate decisions, favoring HF lineaege differentiation over SG differentiation), so perhaps Wnt/beta-catenin dysregulation in general leads to HF miniaturization. But I guess you can't really pin the Cox2 mice results on PGD2 specifically without testing it.
What's interesting is that there's a condition called hypotrichosis simplex, where a certain Wnt inhibitor gene called Apcdd1 doesn't work, and they also suffer HF miniaturization (link). Hmm...
Swoop said:Back to mast cells again, there is also high evidence that they are implicated in tissue remodeling in the body. Well guess what whether one loses hair due to a pathology or whether a healthy hair follicle goes into telogen, the tissue will need to remodel.
This goes back obviously if PGD2 levels are indeed unique to Androgenetic Alopecia but even if it was the other question stands.
However ultimately we can clearly see that even the strongest DP2 antagonists don't seem to provide significant cosmetic changes. I mean take 100 people who all suffer from some sort of degree of Androgenetic Alopecia and place them on dutasteride. A percentage of them will have surely significant cosmetic changes.
This point alone tells me immediately that PGD2 is simply not a major player in the pathology of Androgenetic Alopecia.
The AR however is obviously a major player. And that's what we need to focus on.
Speaking in terms of gene therapy we might be lucky as the AR seems to function as a central role in prostate cancer too
- AZD5312, a generation 2.5 antisense oligonucletotide targeting the androgen receptor
https://clinicaltrials.gov/ct2/show/NCT02144051
Me want. :woot:
- Reaction score
- 1,332
@InBeforeTheCure,
Nice post dude. I'll respond later with some studies. Meanwhile have you looked into estrogen action on the hair follicle? As we know castration + estrogen is pretty much the only thing that can sometimes but not always grow back a considerate amount of hair. I like to quote Cotsarelis in this;
Note also that he says mast cells might contribute to hair loss but I'll get into that later. That's why I made a correlation, to me a increase of mast cells might automatically mean enhanced PGD2 levels as they are the biggest source of that.
Anyway about estrogen, here are two in depth studies; http://press.endocrine.org/doi/full/10.1210/er.2006-0020, http://elib.tiho-hannover.de/dissertations/conradf_ss04.pdf. Curious to your opinion!
Nice post dude. I'll respond later with some studies. Meanwhile have you looked into estrogen action on the hair follicle? As we know castration + estrogen is pretty much the only thing that can sometimes but not always grow back a considerate amount of hair. I like to quote Cotsarelis in this;
Voorhees: What is the mechanism that accounts for the miniaturization of hair?
Dr. Cotsarelis: We know that inhibiting the testosterone pathway slows down the miniaturization of the follicle. Jaworsky, Kligman, and Murphy had a paper 20 years ago showing that half the time there is also inflammation around the hair follicle, which led to some thought that maybe inflammatory cells including mast cells were contributing to hair loss. Studies and case reports of transgender operations where men become women and receive high doses of estrogen show that a scalp that was almost completely bald can have, after castration and high estrogen supplementation, a tremendous amount of hair growth.
Note also that he says mast cells might contribute to hair loss but I'll get into that later. That's why I made a correlation, to me a increase of mast cells might automatically mean enhanced PGD2 levels as they are the biggest source of that.
Anyway about estrogen, here are two in depth studies; http://press.endocrine.org/doi/full/10.1210/er.2006-0020, http://elib.tiho-hannover.de/dissertations/conradf_ss04.pdf. Curious to your opinion!
- Reaction score
- 1,063
Well what about genes? How many studies have outlined the importance of the androgen receptor gene in relation to androgenetic alopecia? Countless! We are unlucky with the inheritance of our genes, some are more lucky. Go read the Hamilton studies.
I don't get what you mean by "it's not just androgens". If everyone would be castrated at a young age on this forum everyone would retain his hair pre-balding and not suffer from Androgenetic Alopecia. Androgenetic Alopecia is dependent on androgens, no wonder as androgens need to exert their biological function through the androgen receptor. Androgens > AR.
I don't see how anything can be more beneficial against Androgenetic Alopecia than total androgen ablation or removal of the AR. Castration stops the progression of Androgenetic Alopecia, so it eliminates the chain of Androgenetic Alopecia.
If we can get gene therapy on our scalp that destroys the AR then that would be the best therapy ever man. Nobody would ever have to suffer from Androgenetic Alopecia again, it's that simple.
Indeed it won't yield reversal of Androgenetic Alopecia, but reversal of Androgenetic Alopecia is something else. Instead of stopping the chain (prevention) you are trying to reverse the action or damage that has been done already. Now that is on a whole different level right..
If you were to be castrated at a young age you wouldn't be here man. You would retain your hair pre-balding.. We all would.
the important DHT for hair is made in itself parting from cholesterol, castration don't stop the production of DHT in scalp hairs.
the important DHT for hair is made in itself parting from cholesterol, castration don't stop the production of DHT in scalp hairs.
Castration stops male pattern baldness completely. If I remember right it not only drops systemic DHT by a ton but it also drops T by a ton. I personally still think lowering T a lot would help with preventing male pattern baldness and its not just DHT. So whether DHT is made in the hair or not doesnt matter. It lowers it systemically by a huge amount so I guess what happens locally there is not significant enough if what you say is true. Also tons of less T means less DHT locally there anyway
- Reaction score
- 1,063
"Castration stops male pattern baldness completely"
This is your idea abcdefg...., but not all people think that Hamilton's investigation are 100% true.
Do you know any study regarding this issue different from Hamilton?
With all due respect.
This is your idea abcdefg...., but not all people think that Hamilton's investigation are 100% true.
Do you know any study regarding this issue different from Hamilton?
With all due respect.
"Castration stops male pattern baldness completely"
This is your idea abcdefg...., but not all people think that Hamilton's investigation are 100% true.
Do you know any study regarding this issue different from Hamilton?
With all due respect.
Do you need more proof than hamilton already gave us? I mean there is real world proof look at castrated men or the pseudo herms that lacked the 5-ar 2 enzyme that finasteride was based off of. Do lots of women grow beards and back hair where your from? Androgens fit the hole perfectly as to why men go bald as they get older because hormone levels naturally change. Yes there is a ton more related to it and many many questions still to answer, but the theory fits. There is nothing to prove for me so believe it or dont. Doesnt matter to me if someone wants to think the world is flat.