
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Topical JAK inhibitors definitely work for androgenic aloipecia -- Big Development
- Thread starter kigoma
- Start date
- Reaction score
- 1,332
Out of context.
He simply refers to the data from Christiano et al. that was performed on a rodent model, and refers to the interesting aspect of it (topical vs systemic). Immediately after he speaks of vitiligo and actual case reports (humans).
He simply refers to the data from Christiano et al. that was performed on a rodent model, and refers to the interesting aspect of it (topical vs systemic). Immediately after he speaks of vitiligo and actual case reports (humans).
- Reaction score
- 1,332
A study in rodents is meaningless really
+1
The fact that he mentions they will release it for Androgenetic Alopecia, as well as the slide near the end mentions topical JAK inhibitors for Androgenetic Alopecia (pg.17). That's promising.
This is what he says pretty much at around 13 minutes;
“We will be developing a topical JAK inhibitor for androgenetic alopecia, and the data on that is quite interesting in that they found that the systemic JAK inhibitor does not work for that particular indication, but the topical does, mainly as a function of the target being more superficial in the skin and not really accessible from a systemic circulation. In vitiligo we have already seen a number of case reports demonstrating the utility of jak inhibitors...."
With "they", he refers to Christiano et al. (Columbia University).
distracted
Established Member
- Reaction score
- 141
Well I was going to say how big a breakthrough this could be, but swoop seems to be saying its just the usual song and dance. Probably wont work that well if at all, and 10 years away if ever.
A study in rodents is meaningless really
Swoop's clearly very knowledgable on this, and I have a lot of respect for what he brings to these forums but I think even he would concede that he doesn't know everything. There is no way he can say with 100% certainty that JAK or a refined formulation of JAK could not work for Androgenetic Alopecia. The comment section of that post seems pretty optimistic. There must be huge overlap between the commentators there and the posters here though.
- Reaction score
- 3,659
What I got out of it was:
"To start looking and deploying capital against two new indications for us and that is androgenetic alopecia and also vitiligo. We will be developing a topical JAK inhibitor for androgenetic alopecia and the data on that (here clearly meaning on Androgenetic Alopecia) is quite interesting in that they found that the systemic JAK inhibitor does not work for that particular indication (still talking about Androgenetic Alopecia), but the topical does... "
Whether or not they have data on human applications well, they seem pretty confident in that it will work so let's hope it does.
"To start looking and deploying capital against two new indications for us and that is androgenetic alopecia and also vitiligo. We will be developing a topical JAK inhibitor for androgenetic alopecia and the data on that (here clearly meaning on Androgenetic Alopecia) is quite interesting in that they found that the systemic JAK inhibitor does not work for that particular indication (still talking about Androgenetic Alopecia), but the topical does... "
Whether or not they have data on human applications well, they seem pretty confident in that it will work so let's hope it does.
- Reaction score
- 1,332
@distracted, indeed, I could never know for sure. I find it extremely unlikely that JAK inhibitors will work for Androgenetic Alopecia, but we'll see. Clearly evidence is lacking with JAK inhibitors though (outside of mice), and this seems to be taken out of context. Hope it works though!! I would like to add that I don't want to be seen as a authority whatsoever. We are all equal here brahs  unk:.
unk:.
Yeah... I can see how many people would misinterpret this and think that they actually already tried this stuff on Androgenetic Alopecia topically and have seen that this grows hair. But that's not what he means. I'm highly sure of this, because he refers to Columbia University. He also follows up immediately with vitiligo and mentions case reports, which are actual humans. He would have done the same for Androgenetic Alopecia, but he speaks of "data".
And no way in hell that Columbia University or A.M Christiano would trial this stuff on multiple persons, without a registered trial in a "secret" way. Subsequently even if it was a case report it would be all over the news, just like with the AA case report. A.M Christiano didn’t mention anything either in her last interview with Spencer. The guy just probably formulated himself wrongly.
Someone should ask him if he actually refers to human data, just to be sure.
unk:. What I got out of it was:
"To start looking and deploying capital against two new indications for us and that is androgenetic alopecia and also vitiligo. We will be developing a topical JAK inhibitor for androgenetic alopecia and the data on that (here clearly meaning on Androgenetic Alopecia) is quite interesting in that they found that the systemic JAK inhibitor does not work for that particular indication (still talking about Androgenetic Alopecia), but the topical does... "
Whether or not they have data on human applications well, they seem pretty confident in that it will work so let's hope it does.
Yeah... I can see how many people would misinterpret this and think that they actually already tried this stuff on Androgenetic Alopecia topically and have seen that this grows hair. But that's not what he means. I'm highly sure of this, because he refers to Columbia University. He also follows up immediately with vitiligo and mentions case reports, which are actual humans. He would have done the same for Androgenetic Alopecia, but he speaks of "data".
And no way in hell that Columbia University or A.M Christiano would trial this stuff on multiple persons, without a registered trial in a "secret" way. Subsequently even if it was a case report it would be all over the news, just like with the AA case report. A.M Christiano didn’t mention anything either in her last interview with Spencer. The guy just probably formulated himself wrongly.
Someone should ask him if he actually refers to human data, just to be sure.
distracted
Established Member
- Reaction score
- 141
@distracted, indeed, I could never know for sure. I find it extremely unlikely that JAK inhibitors will work for Androgenetic Alopecia, but we'll see. Clearly evidence is lacking with JAK inhibitors though (outside of mice), and this seems to be taken out of context. Hope it works though!! I would like to add that I don't want to be seen as a authority whatsoever. We are all equal here brahs
Have you ever posted a reason why you think that? If so, would you mind linking me to the thread?
JAK inhibitors combined with AA treatment could be revolutionary. JAK inhibitors seem to, essentially, signal the follicles to turn on again. With an AA like finasteride or RU creating a healthy environment I'm pretty excited about the possibility here. If you are old and completely bald you are probably SOL, but if you still have a decent population of stem cells this could work wonders.
Blackber
Experienced Member
- Reaction score
- 604
If this proves to show substantial growth for Androgenetic Alopecia I wonder if we'll be able to get it prescribed off-label as more research comes out and it becomes more well know amongst doctors.
Since it's already a FDA approved drug I'm sure that will help make it a LITTLE easier to get through trials but if they're developing a new type of JAK that's target specific I wonder if they'll have to start trials from ground zero.
Any type of new news is always exciting and welcome.
Since it's already a FDA approved drug I'm sure that will help make it a LITTLE easier to get through trials but if they're developing a new type of JAK that's target specific I wonder if they'll have to start trials from ground zero.
Any type of new news is always exciting and welcome.
Blackber
Experienced Member
- Reaction score
- 604
The more this story develops the more Im leaning towards the topical jak being combined with Follica's method eventually.
Would seem to be a likely possibility.
I remember ready that Follica's method made minoxidil 4x more effective.
The more treatments we have the better off we are, especially since everyone doesn't respond to every single treatment.
- Reaction score
- 1,332
Have you ever posted a reason why you think that? If so, would you mind linking me to the thread?
Because Cotsarelis seems to agree with me; http://edition.cnn.com/2014/06/20/health/baldness-cure-alopecia/
Neither doctor said he believes the drug will work for the common kind of baldness that comes with age. Cotsarelis was adamant about it because male pattern baldness isn't related to the immune system. But King said he thinks conducting more research is worth a try.
Nah joke, that would be a bad reason.
I have several reasons but the following would be probably the most important one. When you go to this study; http://advances.sciencemag.org/content/1/9/e1500973.full
We observed that topical treatment with JAK inhibitors resulted in more robust hair growth than did systemic treatment in AA, likely because it increases the local concentration of drug in the HF microenvironment, allowing both actions to occur.
They probably refer with that to this study; http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4362521/
Which says;
[FONT=&]Next, to test a more clinically relevant route of delivery, we asked whether topical administration of protein tyrosine kinase inhibitors could reverse established AA in mice with kinetics similar to those of systemic delivery. In established disease, we found that topical ruxolitinib and topical tofacitinib were both highly effective in reversing disease in treated lesions (applied to back skin). A full coat of hair emerged in the ruxolitinib- or tofacitinib-treated mice by 7 weeks of treatment (data not shown), and we observed complete hair regrowth within 12 weeks following topical therapy ([/FONT]Fig. 4a,b[FONT=&]). Topical therapy was associated with a markedly reduced proportion of CD8[/FONT][FONT=&]+[/FONT][FONT=&]NKG2D[/FONT][FONT=&]+[/FONT][FONT=&] T cells in the treated skin and lymph node ([/FONT]Fig. 4c[FONT=&]), normalization of the ALADIN transcriptional signature ([/FONT]Fig. 4d[FONT=&]), reversal of histological markers of disease ([/FONT]Fig. 4e[FONT=&]) and correction of the GEDI in all treated mice ([/FONT]Supplementary Fig. 12[FONT=&]). Notably, untreated areas on the abdomen remained alopecic ([/FONT]Fig. 4a[FONT=&] and [/FONT]Supplementary Fig. 13[FONT=&]), demonstrating that topical therapy acted locally and that the observed therapeutic effects were not the result of systemic absorption.[/FONT]
It's likely that they refer to the AA mice model in this case.. Because in this case indeed, a topical formulation showed superiority over systemic treatment in AA mice model. As we can indeed also read from the supplemental material;
Alopecia areata reversal was complete on both the back and belly, although the rate of hair regrowth was slower than with topical administration
It wasn't much slower btw..
But let's assume they actually refer to actual humans that have tried oral formulations (actually published) and topical formulations (not published anywhere) of a JAK inhibitor for AA, from which they found that the oral resulted in more "robust" hair growth.
Well have you looked at actual case reports of people that found success for AA with a JAK inhibitor like tofactinib? Or even the ruxolitinib case reports in the last link?
Look at one example here which I posted recently on this link; https://www.instagram.com/thealopeciaexperiment/
Or at the case report of that guy in the first link where Cotsarelis talks. How can hair growth be more "robust" than that? In both cases it's pretty much rapid complete reversal lol.... So that wouldn't make sense would it. Besides let's assume that indeed they have seen more rapid hair growth in AA on humans with a topical formulation. Then what does it matter? At best it would maybe be a tiny bit faster, but eventually it's about the end result. Complete reversal of in this case AA, as displayed in these case reports.
Now the thing is that drugs have biological activity towards a target right? Finasteride primarily has activity towards the 5ar2 enzyme, and also towards 5ar1 at higher dosages. Just like JAK inhibitors have biological activity towards the JAK enzymes.
Now let's take a look at AA;
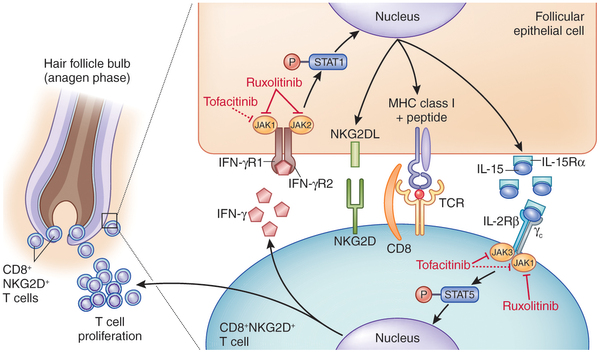
To simplify it in AA, "killer" T cells attack the epithelial compartment of the hair follicle. They hang around the bulb of the hair follicle. So what do JAK inhibitors do? Well they disrupt this process by latching onto these enzymes (which you can see in the above picture). By doing this they disrupt this process which leads to a decrease in these T cells and now the hair follicle is freed to produce a hair shaft again.
The funny thing is.... These killer T cells are around the close proximity of the hair follicle bulb right? So explain to me how these JAK inhibitors can overthrow these JAK enzymes in these T cells in AA (as evidenced by oral AA test subjects) but wouldn't for example on any other cell type in the hair follicle itself? That would be a laughable thing to assume.. And indeed as evidenced in the picture above you see that the picture illustrates that the compound latches towards the enzymes in the follicular ephitelial cells. The same could be said for every cell pretty much of the hair follicle...
Also remember oral JAK inhibitors do not work for Androgenetic Alopecia at the same dosages, period.
All in all there is really no evidence to believe this will do much at all. I'll eat my shoe if this will work and I obviously hope that it will work. But I'll believe it when I'll see it. Not going to get excited from a useless sh*t mice model. Even when you look at that mice model, SAG initiated hair growth just as about as fast as tofactinib so... There would be more, but I'll leave it at this if you don't mind :mrgreen:.
- Reaction score
- 11,939
It's possible that JAK inhibitors do more than affect the immune system.
For example, statins lower cholesterol so people say the benefits of statins are due to lower cholesterol ... but statins actually do a lot in the body other than lower cholesterol.
For example, statins lower cholesterol so people say the benefits of statins are due to lower cholesterol ... but statins actually do a lot in the body other than lower cholesterol.
paleocapa89
Established Member
- Reaction score
- 148
I just want to share this comment here that I found interesting from hlc2020. Maybe people with more scientific knowledge can understand it and have a debate over it:
matt:
This guy seems to know his science, here's another:
matt:
"I agree 100% about IL-6-STAT3 being the main problem… but the question is, is it reversible? I tend to think yes also. Blocking AR, you still have a ton of pathways for IL-6/STAT3 and all of the other bad associated inflammatory agents working through STAT3 to continue the destructive path. The fact that different AR types for asians is not associated with a genetic risk for Androgenetic Alopecia, but the 20p11 SNP next to the FOXA2 gene is the number one at risk spot for them, as well as it being a very close 2nd to the AR for european ethnic people as far as genetic suseptibility to Androgenetic Alopecia, goes to show you that AR/DHT ISN’T OUR MAIN PROBLEM. Across ethnicities 20p11 shows the strongest link to baldness all ethnicities being considered. The FOXA2 gene right next to 20p11 regulates androgen metabolism and IL-6 response amongst many other things. IL-6 (know inflammatory agent) works through STAT3 and STAT3 can associate with cytokines like IL-6 through JAK or other pathways. IL-6 also is associated with PGD2 and DKK1. And STAT3 has been shown to increase Androgen receptor sensitivity and expression in prostate cancer, and even with castration (aka no more AR) STAT3 maintains cancer. STAT3 has also been shown to be a “go” and “stop” signal in different cell populations and when the balance is messed up it can cause cancer. STAT3 over-activation in the bulge makes keratinocyte stem cells change their behavior (look up the article on pubmed from 2015… “constitutive stat3 activation alters behavior of hair follicle stem and progenitor cell populations”). The cells it changes move ABOVE the bulge to and the markers they display are markers for IFE aka skin and cells known to turn into sebaceous gland cells. And JAK/Stat ablation has brought mice and humans back into the growing phase after inflammatory response. Not only this, but 20p11 is associated with a huge risk of idiopathic scoliosis which disproportionately effects adolescent girls, just like early hair loss disproportionately effects guys. A gender specific response on the same gene locus, during a period of growth (puberty). AND THE SAME SNP THAT GIVES THEM THE RISK FOR IDIOPATHIC SCOLIOSIS PROTECTS THEM FROM Androgenetic Alopecia.
What im saying is, it is OBVIOUS what the problem is now. AR susceptibility is just accelerating the process earlier in Europeans that JAK/STAT/IL6 would want to bring about anyways. It is reversibility that is the question. I for one DO NOT want to wait 10 freaking years for this to get through the FDA. Science has been focused on the wrong angle on this question for far too long. Thank god for Christiano’s insight."
This guy seems to know his science, here's another:
"Great finds NASA!!! I read the abstract and briefly browsed through the longer of the two. Will read the entire thing later. I cannot believe that this was that long ago and nothing has been done about it since in regards to Androgenetic Alopecia. We have been slaying the androgen receptor angle for such a long time with such little results. It doesn’t even account for 20% of the variance in Androgenetic Alopecia. And is completely monomirphic in Asians. Their Androgenetic Alopecia is entirely caused by other gene locusts…. And typically occurs on average 10 years later than Europeans. Therefore whatever the mechanism(s) getting turned on in Androgenetic Alopecia are only being excellerated by the bad androgen receptor variant in Europeans. Not directly caused by the androgen receptor. It requires ANDROGENS (specifically DHT) but does not require the specific bad receptor. BIG DIFFERENCE. Looks like Androgenetic Alopecia has a large immune system component just like AA. So many important bits of info not just in these articles… Estrogen inhibits Il-6 and Androgen (especially DHT inducible miRNA-22) stimulates it. This explains why women lose hair at menopause despite declining test levels (bc estrogen protective effect is also declining). IL6 Causes premature Catagen and is induced by DHT in dp cells. Works through stat3 which can oversensitize and over-induce Ar expression. Stat3 is also responsible for the premature cellular senescence of DP (and other cell pops… It is a cancer protection mechanism trying to shut the cell down in the presence of ROS). Overexpression of keratinocyte specific mitochondrial stat3 causes slowed gene expression in direct energy unit of cell… Thus explaining why they cannot re-enter the hair cycle after a certain threshold has been reached… They are exhausted. Loses contact from arector pili…. Stat3 mediates muscle satellite helper cell regeneration…. And too much stat3 retards the process. Stat3 is needed for dkk1 in DP which messes with the beta catenin and Wnt pathways. The information is right in front of your guys’ faces. THIS IS IT AND NASA-RS WAS SPOT ON. They have found the needle in the haystack in my opinion. It’s the same one acting in AA and graft vs host disease… Both of which have stimulated hair growth topically with JAK inhibitors. They just have different patterns and time rates. This is going to work in Androgenetic Alopecia in a high concentration topical with effective delivery."
NorwoodGuardian
Established Member
- Reaction score
- 184
Seems more knowledge than Swoop.
- Reaction score
- 1,332
Seems more knowledge than Swoop.
Again little boys like you who are led solely by emotions. It's pure fear what you have inside, that's why you are blinded by hope. I have seen so many guys like you. They never turned out to be right and they eventually vanished probably in desperation. They would be so extremely sure of their case. It's no different this time mate. Evidence lacks again and there is much hype for nothing. It's a never ending cycle. I can even give you some links, it's pure comedy. Look at my post history on BTH.
False hope is a bad thing brah. This is false hope. Come back when you have anything to show outside of mice models, some evidence in humans you know? Before that you stand nowhere.
So I'll ask you again; EVIDENCE IN HUMANS?!?!?!?! Pictures? Data? Case report?
I want this to work just as well as anyone, but getting hyped up for nothing is f*cking nonsense. It has happened many times before and I still only see finasteride and minoxidil, no? It's tiring, a thing you might understand in a few years from now.